


Do Vaccines Really Reduce Childhood Mortality and Extend Life Expectancy? A Critical Examination of the CDC’s Claims
A critical evaluation of CDC's report on the effects of vaccines on children born between 1994 and 2023. Without considering morbidity and mortality from vaccines, the report is at best vacuous.
This figure, from CDC data, shows a dramatic increase in all-cause mortality in children in the US from 2012 to 2024.

There is little wonder why the public has lost “faith” in CDC. What have they been doing? Where is the return on our investment?
The Centers for Disease Control and Prevention (CDC) identifies the leading causes of death among children in the United States, which vary by age group. Here's a breakdown:
Ages 1–4 Years:
Accidents (Unintentional Injuries): Leading causes include drowning, motor vehicle incidents, and suffocation.
Congenital Malformations, Deformations, and Chromosomal Abnormalities: These are birth defects affecting the structure or function of the body. CDC does not consider vaccination during pregnancy to be a risk factor, yet fetal demise skyrockets if women vaccinate (Shimabukuro, unpublished data).
Assault (Homicide): Deaths resulting from intentional harm by others.
Ages 5–9 Years:
Accidents (Unintentional Injuries): Motor vehicle accidents are prominent in this age group.
Cancer: Various forms of malignancies.
Congenital Malformations, Deformations, and Chromosomal Abnormalities: Ongoing impacts of birth defects.
Ages 10–14 Years:
Accidents (Unintentional Injuries): Including motor vehicle accidents and drowning.
Intentional Self-Harm (Suicide): Mental health challenges leading to self-inflicted harm.
Cancer: Various forms of malignancies.
Ages 15–19 Years:
Accidents (Unintentional Injuries): Motor vehicle accidents are a significant cause.
Homicide: Deaths resulting from intentional harm by others.
Suicide: Mental health challenges leading to self-inflicted harm.
While unintentional injuries are the leading cause of death across these age groups, the specific types of injuries and other leading causes can vary. For instance, in younger children, drowning is a significant risk, whereas in adolescents, motor vehicle accidents and firearm accidents rank highest, both of which could reasonably be related to syncope or reduced reasoning ability (think: aluminum, mercury, and fluoride interactions).
These statistics underscore the importance of targeted prevention efforts, such as promoting safe driving practices, ensuring safe storage of firearms, providing mental health support, considering the effects of vaccination and fluoride on cognition reasoning and logic, and implementing safety measures around water to reduce the risk of drowning.
CDC’S VACCINES HAVE PREVENTED 1.1M DEATHS REPORT
Vaccination has long been credited as one of the most effective public health measures in modern history, with claims that it significantly reduces mortality and extends life expectancy. The Centers for Disease Control and Prevention (CDC) recently published a report in the non-peer reviewed publication Morbidity and Mortality Weekly Report (MMWR), asserting that routine childhood vaccinations have prevented approximately 1,129,000 deaths among children born between 1994 and 2023. Roughly speaking, that is about 1.2% of all deaths from all causes over the same time period. For unstated reasons, CDC left out RSV, influenza, and COVID-19 vaccination from their analysis.
But are these mortality reductions based on empirical observation, or are they the result of extrapolated models and assumptions? This article critically examines the CDC’s claims, evaluates the evidence presented, and explores the broader context of mortality reduction in modern public health.
How the CDC Calculates ‘Lives Saved’
The CDC’s report does not rely on direct mortality data but instead employs economic and epidemiological models to estimate the number of deaths prevented by vaccines. The key methodological steps include:
Using pre-vaccine era data on disease incidence and mortality to estimate the number of deaths expected in the absence of vaccines.
Applying vaccination coverage rates over time to project how many people would have developed the disease.
Ignore that many vaccines do not prevent transmission.
Using mathematical decision-tree models to estimate how many of those cases would have resulted in hospitalization and death.
Claiming the difference between projected deaths and observed deaths as ‘lives saved’.
Ignore completely any potential effect of mercury and aluminum on total health risks.
While modeling is a standard approach in epidemiology, it is only as accurate as its underlying assumptions and data sources. A closer look at these models reveals significant limitations.
Key Weaknesses in the CDC’s Approach
Mortality Reduction is an Extrapolated Estimate, Not an Observed Reality
The 1.1 million deaths prevented claim is not derived from direct hospital records or death certificates, but rather from extrapolated models. This is problematic because it assumes:
Disease mortality rates in infants under 1 year old (vaccinated and unvaccinated) populations remain constant, even though modern medical advancements (e.g., antibiotics, ICU care, better nutrition) have dramatically improved survival rates.
Natural immunity acquisition is ignored, meaning people who acquire and recover from infections without vaccination are not factored into mortality reductions.
Serotype replacement and viral evolution are excluded, failing to account for how pathogens adapt in response to mass vaccination.
Thus, the lack of real-world mortality tracking weakens the certainty of the CDC’s claims.
The Report Does Not Use Hospital Death Data or Longitudinal Mortality Tracking
Despite making strong mortality reduction claims, the CDC report does not include direct observational mortality data. Instead, it relies on:
National Notifiable Diseases Surveillance System (NNDSS) – Tracks reportable diseases but does not systematically track deaths.
Active Bacterial Core Surveillance (ABCs) – Focuses on bacterial infections only, meaning viral diseases (measles, rubella, varicella) are modeled, not observed.
National Immunization Surveys (NIS) & School Vaccination Surveys – These provide vaccination coverage rates, but do not track disease outcomes or mortality.
This raises serious concerns: If direct mortality tracking was performed, would the numbers match the modeled projections? Without an observational study, the CDC’s claims remain theoretical.
The Assumption That All Deaths Would Occur Without Vaccines
The CDC assumes that, without vaccines, vaccine-preventable diseases would still cause the same number of deaths as they did in the early 20th century. This assumption is flawed because:
Medical advancements such as antibiotics, antivirals, and ICU care significantly reduce mortality.
Supportive treatments (e.g., rehydration therapy for rotavirus, ventilators for severe pneumonia) save many patients who would have died decades ago.
Improved sanitation and hygiene reduce disease transmission, independently of vaccines. To their credit, their report did include: “(F)or some diseases, factors other than immunization (e.g., hygiene and physical distancing measures) might have contributed to lower disease risks in recent decades, and reductions resulting from these contributions have not been incorporated into the model.”
For instance, measles deaths had already fallen by over 90% before mass vaccination due to these public health improvements. The CDC’s model attributes all mortality reduction to vaccines, but this ignores other critical factors. CDC’s report does not provide WHO’s recommendation of two high doses of Vitamin A in measles cases to reduce the severity of symptoms.
The Role of Other Public Health Improvements in Reducing Mortality
The CDC report fails to acknowledge that many vaccine-preventable diseases were already declining before vaccines were introduced due to:
Better sanitation and clean water initiatives reducing exposure to infectious agents.
Antibiotic use, drastically reducing complications from bacterial co-infections.
General improvements in healthcare accessibility, increasing survival rates for those who contract diseases.
Declining birth rates, which reduce transmission in smaller family units.
The absence of these factors in the CDC’s model overestimates the role of vaccination in mortality decline.
The Economic Claims: Are They Inflated?
The CDC claims that childhood vaccinations have resulted in $2.7 trillion in societal savings, primarily from:
Projected lost productivity from premature deaths avoided.
Treatment costs averted by preventing illnesses (ignoring that many vaccines do not prevent transmission).
Indirect benefits such as reduced caregiver burden.
However, this analysis ignores key economic factors:
It assumes that all deaths prevented would have led to equivalent economic productivity, which is an unrealistic assumption.
It does not account for vaccine injuries, which carry their own medical and legal costs and costs in terms of morbidity and mortality, and massive economic burdens on families.
It assumes vaccines are always effective, disregarding so-called “breakthrough infections”, waning immunity, and evidence of higher likelihood of respiratory infections following inactivated influenza vaccination.
A more balanced economic assessment would account for both benefits and costs, rather than focusing solely on potential savings.
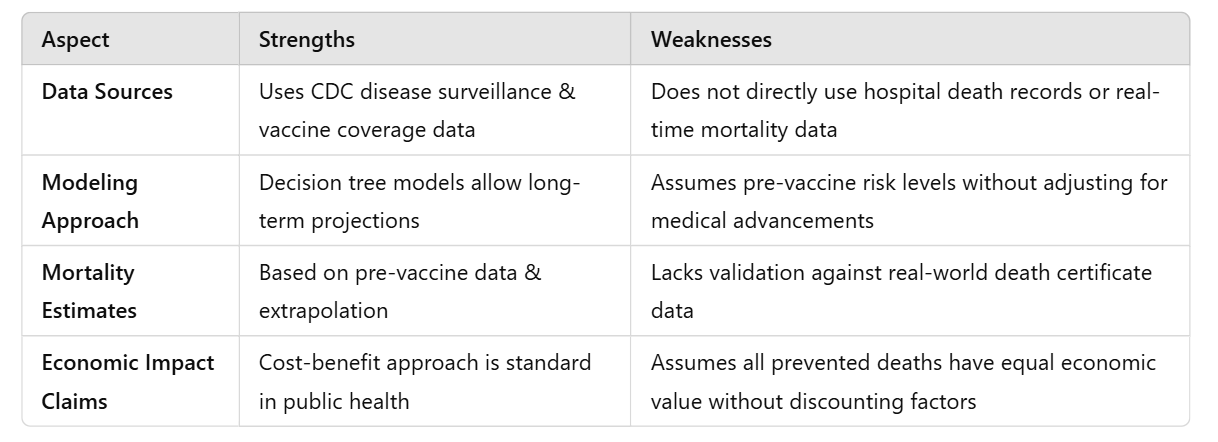
Summary of the Strengths and Weaknesses of the CDC Report
To further clarify the issues, the following table outlines the key strengths and weaknesses in the CDC’s approach:
The Nuanced Reality: Do Vaccines Reduce Mortality?
PERHAPS, But Not as Dramatically as the CDC Claims
Their exact effect of vaccines on morbidity and mortality using CDC’s approach is difficult to quantify because:
Other public health advancements have played a major role in mortality decline.
The CDC does not directly track real-world deaths prevented, only models them.
Vaccine effectiveness varies by disease, population, and time.
A more accurate statement would be that SOME vaccines MAY CONTRIBUTE to reducing mortality, but their effect is often overstated when other factors are ignored, and that more direct research is needed - such as the Lyons-Weiler and Thomas study, which was wrongfully retracted by the journal IJERPH.
What a More Accurate Analysis Would Require
To produce a more rigorous and reliable assessment, future studies should:
Use direct mortality tracking from hospital records, rather than relying solely on model projections.
Include the direct study of total health outcomes associated with vaccine exposure so morbidity and mortality usually (systematically) not associated with vaccine exposure can be factors.
Account for public health improvements like sanitation and antibiotics in assessing mortality reduction.
Perform sensitivity analyses to explore how changes in vaccine effectiveness or medical advancements affect outcomes.
Consider vaccine breakthrough infections, waning immunity, and increased risks of infections, in contrast to lifelong protection from a single infection.
Without these improvements, claims of ‘millions of deaths prevented’ remain speculative and theoretical rather than empirically verified.
Conclusion: A More Balanced Perspective on Vaccines and Mortality
Vaccines play an important role in reducing disease burden, but the CDC’s claim that vaccination alone is responsible for 1.1 million fewer deaths is based on models, not direct observation. The lack of mortality tracking, reliance on pre-vaccine mortality rates, and exclusion of other public health advances suggests that these estimates are potentially vastly inflated.
A more rigorous, evidence-based approach is needed—one that incorporates real-world death tracking, sensitivity analyses, broader public health factors and total health outcome. If public trust in vaccines is to be maintained, transparency and empirical validation must take precedence over modeled assumptions.
The Film Rain Man Was Likely Forged to Pre-Program the Populace For the Upcoming Explosion in Vaccine Induced Autism.
1986: Congress Grants Immunity Shield to Vaccine Makers for Venom Injection Damage | Film Rain Man Begins Production
1988: Rain Man Released to Educate, Condition, & Normalize Autism
1986—2025: Number of vaccines administered explodes to 78 - and rising - from birth to two years of age. Autism diagnoses explode right along with them.
Before the film few even knew what the term meant because it was so rare it was seldom reported: https://tritorch.substack.com/p/autism-pre-conditioning-and-normalization
Brilliant as always, Dr. Jack. As thoroughly as you have dismantled the overall premise, how reliable is the opening line in the conclusion? "Vaccines play an important role in reducing disease burden." For example, once the measles vaccine was introduced after the (modeled) disease burden had already dropped by 90%, couldn't the remaining 10% improvement be matched and even exceeded by the damage caused by the vaccines? Especially given that high dose Vit A prevents complications from the measles. Why be so generous towards the clan of needles? It seems to me they still haven't really proven that anything positive can be attributed to their campaigns.