


Who Are the World's Leading Authorities in COVID-19 Treatment?
Public Health's "Medicine" is to go home and wait until you get sick (No Treatment Protocol). That is utterly unethical.

James Lyons-Weiler, PhD - 9/27/2021
At the onset of the COVID-19 pandemic, the mantra was “flatten the curve”. I had already done simulations showing that given the epidemiological parameters of COVID-19, its R0 in particular, that a multimodal approach would be necessary to bring the number of new cases down to a non-scary level. “A low buzz”, I called it, and one of the things I modeled was treatment.
I did this when we were told that the mortality rate among people with co-morbid conditions, like diabetes, was around 20%. It was also before the number of cases were polluted with data including false positives, and “presumed COVID” cases, in which doctors overrule negative tests, or give a diagnosis of COVID-19 without any confirming test. This was before CDC made the economy-crushing near fatal error of conflating “PCR positive” with “COVID-19” and the likewise unscientific “Died with = Died From”. Given our intended success in moving a grand jury investigation forward in Oregon on CDC's failure to follow protocols for changing diagnostic and reporting criteria, there will almost certainly be a reckoning on that point.
By now, 9/27/2021, everyone has heard of Ivermectin, in large part due to Joe Rogan’s use of the FDA-approved drug, and of Hydroxychloroquine, in large part due to its support by Donald Trumps support of the FDA-approved drug and its subsequent politicization. The fact is, these and other treatments were found to be effective by the first step in science – observation. In the US, off-label use is permitted for a potentially fatal condition when no standard of care exists. When Dr. Peter McCullough, and Dr. Pierre Kory, and Dr. Paul Marik used observation to conclude that perhaps certain approaches to treatment might save lives, they acted. There was no standard of care; they recognized that there was no approved drug for treatment of COVID-19, so they appropriately reported their own, and others’ finding.

In highly vaccinated countries, the number of new cases is at an all-time high. People are still dying from COVID-19. And there is still no approved drug to treat COVID-19.
The problem is clear: the information on effective treatments is not getting to doctors.
Doctors are required to read materials sent to them by the US government. The failure of the regulatory agencies to back in-home ambulatory and early treatment has created a world in which the number of people with high viremia is unacceptably high. The untreated are incubators of new variants - and yet these agencies are now mostly mute on available treatments supported by science.
What would an expert case for the use of the well-studied treatments look like? For that, we can turn to Drs. McCullough and Vijay.

Under the conditions where the benefit to the individual is clear, in-home ambulatory treatment makes sense. See the figure above from McCullough and Vijay (2021). Under this view, when individual and population interventions do not occur, and people are told to quarantine and get sick, the immediate need for hospitalization is stemmed, but over time, bad things happen. When individual and population interventions are numerous and multi-faceted, the need for hospital care is minimized and good things happen - more people recover.
FLCCC Alliance also have protocols - well-reasoned, back by observation, real-world data, clinical studies and meta-analyses - that all physicians should read. These are the IMASK+, MATH+, and I-RECOVER protocols, along with a Complete Guide to the Care of the COVID-19 Patient.

When antivirals save lives, they do so by their therapeutic effect of keeping viremia - the amount of virus present in a patient’s body, down. This not only has benefit to the individual - it also reduces the rate of transmission. Allowing people to go home and become veritable incubators of the virus until they are close to death is of no benefit to the individual, and places people around that person at risk of infection, for a needlessly protracted period of time.
Dr. McCullough and colleagues long ago formalized a multi-faceted treatment for people who test positive for COVID-19 based on their understanding of how the virus causes disease.
Their multi-faceted approach comes with a decision flow diagram, backed by clinical experience and real-world data, which is increasingly being viewed by physicians as a viable protocol for in-home care.
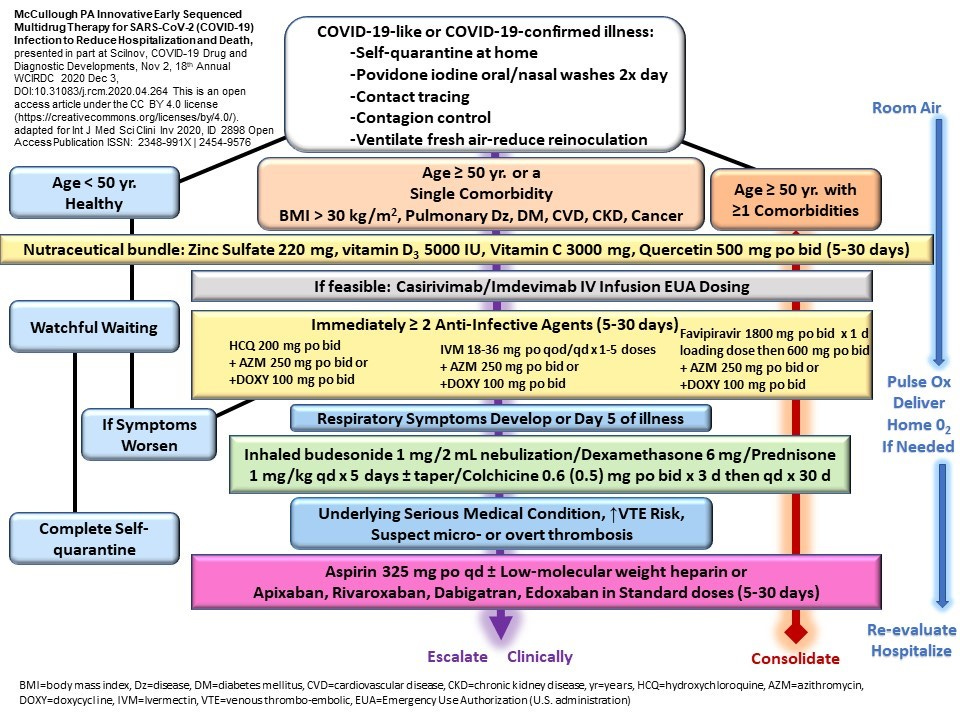
Makes sense, right? This is infinitely better than telling people to go home and incubate.
What does not make sense is why studies that alleged to show that treatments do not work focused on late-stage COVID-19 patients, and, as Dr. Meryl Nass pointed out, used fatal doses. One study used to turf Hydroxychloroquine published in The Lancet was found to be utterly fraudulent. Knowing what you now know about FDA’s conditions for off-label use, the messaging from FDA that Ivermectin is “not approved” for treatment of COVID-19 seems toothless, but not harmless. And Fauci’s claim that the Henry Ford study was not impressive because patients had received both corticosteroids and hydroxychloroquine was disingenuous at best. Fauci should have celebrated the 50% reduction in mortality and called for more studies; instead, he was content to bury treatment and condemn untold thousands of patients to go home until they get sick enough for emergency care.
AAPS has an in-home treatment protocol as well, with a guide authored by Dr. Jane Orient and Dr. Elizabeth Lee Vliet.

The world’s leading experts on COVID-19 treatment protocols are authorities like Dr. Peter McCullough, Dr. Pierre Kory, Dr. Jane Orient and Dr. Elizabeth Lee Vliet. I had interviewed Dr. McCullough on Unbreaking Science over year ago, on Sept 15, 2020, and Dr. Kory on January 16, 2021. I interviewed Dr. Orient on December 15, 2020. Others include Dr. Zev Zelenko and Dr. David Brownstein - all early voices on lowered death rates and faster recovery times associated with COVID-19 ambulatory treatments. I interviewed Dr. Brownstein but did not manage to interview Dr. Zelenko - yet. The information from the world’s leading experts on COVID-19 treatment has been actively suppressed via the usual outlets, so I’m not surprised you missed these interviews.
So Who Are the Authorities?
So who are the world’s leading experts in the care of COVID-19 patients? Bureaucrats at the FDA? Public health personnel at the CDC? Fauci? Not by a long shot. They have so negatively influenced the COVID-19 pathway in the US they must be removed from office - immediately - and replaced with true medical authorities.
The Problem is Censorship and Regulatory Capture. The Solution is YOU.
The problem is that this information is not getting to doctors. So it’s up to you to send this key information to physicians and challenge them to read it carefully.
The answer to active censorship and suppression is YOU.
Take the message directly to all physicians you know - and ask them two questions:
(1) Have they adopted any of these rational approaches to in-home ambulatory care, and if no, then
(2) Why?
Physicians are taught and socialized to respect authority. The doctors whom I recognize as authorities in treatment do not seek authority. But you must nevertheless grant it to them, and they must, even if begrudgingly, accept the role. If your patients are dying, you must - MUST - defer to those people who are seeing their patients thrive and survive. If you are an ethical physician, you can join thousands from around the world who have signed The Rome Declaration, a Physicians Statement - and invite your colleagues to say no to needless disease and death under public health’s vision of COVID-19 medicine of going home until you’re sick enough for emergency care. Get on the medical board and push for a change in COVID-19 standard of care.
If you’re in doubt, realize this: there has never been a large, long randomized clinical trial that shows that “go home until you are near death”; i.e., no care at all, is more effective that the emerging de facto standards of care.
If you are an unethical physician, please leave medicine and leave it to the experts.
If you an ethical American citizen, demand a Senate hearing on why Fauci and others currently sitting in key positions in regulatory and governmental research agencies knowingly sent - and continue to send - hundreds of thousands of your fellow Americans home without medical care. Demand their resignation or termination. Then we can begin to build back better.

Watch Dr. McCullough, one of the world’s foremost authorities on the treatment of COVID-19, break down for a very interested public all that has gone wrong with the US public health response to COVID-19. A panel discussion follows.
References
McCullough et al., 2021. Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection. Am J Med https://www.amjmed.com/article/S0002-9343(20)30673-2/fulltext
Orient, J and Vliet, EA. A Guide to Home-Based COVID Treatment Step-By-Step Doctors' Plan That Could Save Your Life. AAPS Online https://aapsonline.org/CovidPatientTreatmentGuide.pdf
FLCCC Alliance. An overview of the MATH+, I-MASK+ and I-RECOVER Protocols A Guide to the Management of COVID-19 https://covid19criticalcare.com/wp-content/uploads/2020/12/FLCCC-Protocols-–-A-Guide-to-the-Management-of-COVID-19.pdf
Lenze et al., Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19 A Randomized Clinical Trial https://jamanetwork.com/journals/jama/fullarticle/2773108
You have given the wrong organization credit for a list of protocols. As you wrote <<America’s Frontline Doctors also have protocols - well-reasoned, back by observation, real-world data, clinical studies and meta-analyses - that all physicians should read. These are the IMASK+, MATH+, and I-RECOVER protocols, along with a Complete Guide to the Care of the COVID-19 Patient.>>
It is FLCCC that has produced those protocols, not America’s Frontline Doctors. Two very different organizations. Please correct this.
Exactly. Thank you for your perseverance. It is having an impact!