


The Evidence for Unacceptably High False Positive Rates is Overwhelming
The dark stain of false positives: Screening with RT-PCR was a disaster in the making from Day 1. Full-length IPAK False Positive report included.

When I testified on a case in Pennsylvania, I proffered citations from the peer-reviewed scientific literature that provided COVID-19 false positive rate estimates from RT-PCR test kits in use for diagnosis. After I sent my written testimony to the defendant’s lawyers, the written testimony from a State Epidemiologist was sent to me. It contained the stunningly incorrect claim that the use of RT-PCR in the diagnosis of COVID-19 was free from false positives.
Somehow, via the comparison of my testimony and hers, the judge on the case became convinced to only accept verbal testimony.
The restaurant lost the case, but the scientific literature remains.
Few people realize that false positives rates as high as 11% were known fairly early on. In December 2020, an Australian team reminded the world that when the prevalence of a condition or disease is low, false positives can lead to costly errors that outnumber the number of true positive cases. That article, “Accuracy amidst ambiguity: false positive SARS-CoV-2 nucleic acid tests when COVID-19 prevalence is low”, was one that I had cited in my testimony. (Low prevalence is why we don’t do cancer screens routinely with PET-scans because the number of deaths due to infection following biopsy in false positive “patients” will outnumber the number of lives saved by detection of cancer via PET-scan screening).
Another study I had cited was the Marine study. In the Marine study, a cohort of Marine recruits - isolated on an otherwise emptied college campus - were tested via PCR routinely. Those who tested positive via PCR were removed. The study authors reported that they had “obtained more than 95% complete viral genomes from 36 specimens obtained from 32 of 51 participants (62.7%) who had positive qPCR results for SARS-CoV-2”.
To me, this implies a 37.3% false positive rate; the samples from the Marines used to attempt to derive full SARS-CoV-2 genomes were obtained on the same day as the PCR test, and failure to be able to derive sequence means the virus was not present.
Cohen et al. wrote "(E)vidence from external quality assessments and real-world data indicate enough a high enough false positive rate to make positive results highly unreliable over a broad range of scenarios. This has clinical and case management implications, and affects an array of epidemiological statistics, including the asymptomatic ratio, prevalence, and hospitalization and death rates, as well as epidemiologic models."
And they also outline how "SARS CoV 2 Mass Testing Endangers Residents of Long-Term Care Facilities" due to false positives.
A very clear-cut description of the problem is published in the Journal of Occupational and Environmental Medicine, in which the authors correctly contract the risk of false positives of RT-PCR for COVID-19 in the symptomatic compared to the screening setting. While the risk is lower if the testing is limited to the symptomatic, or those known to be exposed the authors correctly state:
“Doing these same calculations for the screening scenario, 100 of the 10,000 individuals are infected and 9900 are not. The test will detect 95 of the infected persons and five will be falsely negative. For those who are not infected, 9702 will be correctly diagnosed and 198 will be false positives. The PPV is 95/95 + 198 or 32.4%. In this case, 2/3 of the positive results are false positives. For a prevalence of 0.1%, the PPV drops to 4.5%.”
See: False Positive Results With SARS-CoV-2 RT-PCR Tests and How to Evaluate a RT-PCR-Positive Test for the Possibility of a False Positive Result. Journal of Occupational and Environmental Medicine 63:e159-162 doi: 10.1097/JOM.0000000000002138
These authors also provide a table of costs of false positives:
TABLE 2 - Impacts of False Positive Results (Modified and extended)
Unnecessary isolation of individuals and quarantining of close contacts with financial and psychological strains
Unnecessary contact tracing and testing
Delays in surgical or other procedures
Prolong hospital stays, with wasteful consumption of PPE
Potentially harboring uninfected individuals with infected individuals in hospitals and congregate living areas with possible nosocomial infection
Possible exposure to inappropriate medical treatment
Individuals given false sense of security about their (false) immunity, so may not follow public health guidelines
Impede correct diagnosis of patients with symptoms
Overdiagnosis may distort epidemiologic statistics by including false-positives to estimate prevalence, hospitalization, and death rates as well as modeling (eg, some individuals classified as asymptomatic carriers may actually had a false positive test).
Twitter is filled with tweets enumerating the #CostoftheFalsePositive.
Dr. Sin Hang Lee (Millford, CT) estimates that the diagnosis rate via PCR is grossly exaggerated and that the FPR of the use of RT-PCR as implemented in the diagnosis of COVID-19 may be as high as 91%.
He points to a table published in a Supplement to a retrospective cohort study published in Lancet in 2021 (Tartof SY, Slezak JM, Fischer H, et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet 2021; published online Oct 4. http://dx.doi.org/10.1016/S0140-6736(21)02183-8):
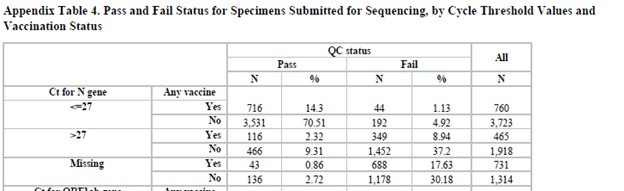
From this table, the FPR can be estimated as
(688+1178)/(731+1314)= 1866/2045= 91%
If verified, this means that the mortality rate estimates cited by CDC and others, including OSHA, are likely to have been woefully incorrect.
It would also mean that the efficacy of the vaccines is not well-determined given that the COVID-19 status in the trials were based on experimental use of RT-PCR with a fixed cycle threshold as a proxy diagnosis of COVID-19 under an Emergency Use Authorization.
A more recent study, published in JAMA, blithely reported a massive, 62% false positive rate in antigen tests).
It is lamentable that so-called Fact Checker narrative minders attacked independent, objective research on the important question of false positives. The ad hominem on my reputation by the lawyer in the Pennsylvania restaurant case using a misguided Special Master’s decision to ignore my two decades in Biomedical Research betrayed the tactic “when you can’t attack the message, attack the messenger”.
So far, such attacks only seem to bolster public support for my independent research. IPAK has now funded Dr. Sin Hang Lee (along with a matching grant from EWI) to provide an additional estimate of false positives present in so-called gold standard validation technical samples.
Dr. Lee is having difficulty getting journals to publish his damning results, because they demonstrate that RT-PCR testing is a train wreck overall. A prior study by Dr. Lee revealed 30% false positive and 20% false negative (see Bloomberg). The samples he analyzed were a reference set by which laboratories were supposed check their nucleic acid test results against for accuracy. Dr. Lee’s technique is to use nested PCR primers so he can see when a mutation or mutations in the primer sites are causing PCR test drop-out, which leads to a 50% reduction in sensitivity of these tests (the ability to detect the virus when it is, in fact, present). He can also provide sequences that characterize specific variants - all using good old-fashioned Sanger sequencing.
The denialists will deny and continue to put a stranglehold on reality. In the meantime, lives are put on hold, cases and death counts are unreliable, and people who believe they had COVID-19 and are now testing positive again either never were positive, are not now positive, or both never were and are not now truly positive. “Reinfection” rates are therefore skewed.
RT-PCR was never meant to be used with a single cycle threshold; each individual test is supposed to be run with one or more controls, allowing the detection threshold to be estimated. We have an email from HHS acknowledging that any test result >35 cycles is basically useless, yet by various means (all legal), we have determined that the cycle threshold commonly in use has been over 35. Medical doctors and public health agencies (state and Federal) have all kept the cycle threshold being used close to their chest, citing that they were proprietary - a crock of baloney because even using a single cycle threshold with RT-PCR is bogus.
One of the IPAK projects from 2021 was to model the COVID-19 diagnosis given all of the policy positions adopted, from “PCR+ = COVID-19” (bogus) to “Died With = Died From” also bogus, and in the middle some PCR false positives. This modeling effort took extreme effort, and, well, since four public health journals refused to publish it, I’ll make it available here, not peer-reviewed, but certainly ready for prime time. [LW/IPAK Sisyphean Effort PCR Report]. The take-home? Under CDC’s testing/diagnosis/death determination paradigm unilaterally thrust on an unsuspecting US public, the more RT-PCR testing that gets done, the higher the false positive rate.
We’ve been proven right. By “we”, I mean IPAK, people like Dr. Ealy and colleagues published in the IPAK journal, Dr. Sin Hang Lee, Dr. Scott Jensen, and anyone else warning that RT-PCR false positives will obscure signals and prevent the production of credible data on cases and deaths. The over-reporting in cases and death is not merely due to the reliance on RT-PCR: it’s also due to the resistance by FDA and CDC to foster RNA Sequencing-Based diagnostics, which when done right would completely clarify the situation (well, almost. The presence of the virus does not mean it is causing disease, and its presence certainly does not confirm itself as the cause of death).
USAToday, Reuters, Politifact, Fact-Checks-R-Us (that’s not real) and all the other narrative minding, blog opinion article websites that tout themselves as “Fact-Checking” sites should address the advances in knowledge and issue corrections to their publications that have incorrectly claimed that our understanding of the over-reporting of COVID-19 cases and deaths by CDC were false. This isn’t about reputation. It’s about helping the US come to grips with the scale of the testing fiasco, and its cost to society.
The establishment’s disregard and disdain for empirical evidence of false positives in PCR testing are deplorable.
So we’ll continue to educate and inform.
To pitch in and help IPAK do and fund independent biomedical and public health research, follow this link, click on Monthly (Science Hero), and I thank you.


It was obvious from the get-go because they were testing asymptomatic people for an acute respiratory infection, contra every other case definition for ARIs, which always start with compatible signs and symptoms that are confirmed by testing. Bayes' Theorem, anyone? Thought experiment using an extreme example to illustrate Bayes' Theorem: If you test biological males for pregnancy, and any turn up positive, are they more likely to be true or false positives? Now the reverse: If you test biological women who appear to be in the end-stages of normal pregnancy, and any turn up positive, are they more likely to be true or false positives?
The emergency room at a local hospital takes a temperature test, if no fever no VOVID! My mom was diagnosed wit bacterial pneumonia, given ZPak and what was funny the COVID 19 seating section was empty, and while waiting 6 hours for her release, not 1 case was diagnosed! Looks like the funds ran out for false positives!