


Progress Report: Reevaluation of Aluminum Exposure in Pediatric Vaccination Schedules
Now that we know that aluminum toxicity in the CDC's schedule leads to chronic toxicity in infancy and early childhood, our next study is ongoing - and needs your support. It's up to you!

Introduction
The safety of aluminum adjuvants in vaccines, particularly for pediatric populations, has been a subject of increasing concern and scrutiny. This progress report aims to summarize and evaluate the contributions made by Dr. Lyons-Weiler and colleagues in this critical area of public health. Their research has focused on the modeling of whole-body aluminum toxicity in the context of the United States pediatric vaccine schedule, providing invaluable insights into the potential risks associated with aluminum exposure.
Methodological Rigor
The studies conducted by Dr. Lyons-Weiler and his team are characterized by their methodological rigor, incorporating both computational and empirical data. Advanced mathematical models, such as Clark’s Rule, Hill's equations and pharmacokinetic modeling, have been employed to provide a nuanced understanding of aluminum toxicity.
Study 1: Reconsideration of the Immunotherapeutic Pediatric Safe Dose Levels of Aluminum
The first study by Lyons-Weiler and Ricketson is a reconsideration of the immunotherapeutic pediatric safe dose levels of aluminum. We estimated a pediatric dose limit that considers body weight and identify several serious historical missteps in past analyses of provisional safe levels of aluminum in vaccines. We concluded that the levels of aluminum suggested by the currently used limits place infants at risk of acute, repeated, and possibly chronic exposures of toxic levels of aluminum in modern vaccine schedules[1].
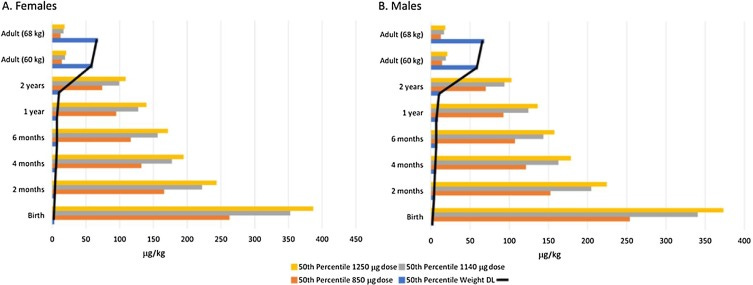
We employed a Pediatric Dose Limit model that considers body weight and identifies several historical missteps in the analysis of provisional safe levels of aluminum. The study concludes that the current vaccine schedule may expose infants to toxic levels of aluminum, particularly when body weight is considered. Specifically, the study found that aluminum doses, when estimated from Federal Regulatory Code given body weight, exceed the weight-corrected Pediatric Dose Limit[1] leading to whole-body toxicity that appears to chronic over long periods of infancy and early childhood.
Study 2: Acute Exposure and Chronic Retention of Aluminum in Three Vaccine Schedules
The second study by McFarland et al. explored the expected acute exposures and longer-term whole-body accumulation/clearance across three vaccination schedules: the current US Centers for Disease Control and Prevention (CDC) schedule, the current CDC schedule using low aluminum or no aluminum vaccines, and Dr. Paul Thomas’ “vaccine-friendly plan” schedule. We then studied the effects of an implicit assumption of the priest model on whether clearance dynamics from successive doses are influenced by the current level of aluminum or modeled by the assumption that a new dose has its own whole-body dynamics “reset” on the day of injection. We modeled two additional factors: variation (deficiency) in aluminum detoxification, and a factor added to the priest equation to model the potential impact of aluminum itself on cellular and whole-body detoxification. These explorations were compared to a previously estimated pediatric dose limit (PDL) of whole-body aluminum exposure and provide a new statistic: %alumtox, the (expected) percentage of days (or weeks) an infant is in aluminum toxicity, reflecting chronic toxicity. We showed that among three schedules, the CDC schedule results in the highest %alumtox regardless of model assumptions, and the vaccine-friendly plan schedule, which avoids >1 aluminum-containing vaccines per office visit results in the lowest (expected) %alumtox2.
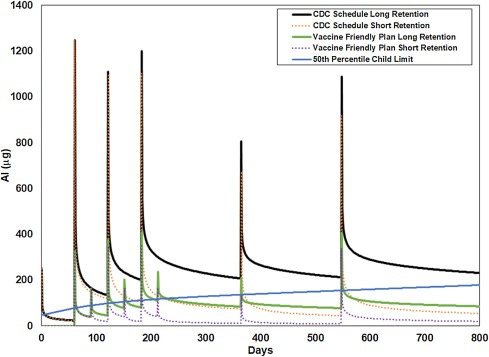
This study explored the acute exposures and longer-term whole-body accumulation of aluminum across three vaccination schedules. It also considered the effects of genetic and environmental factors on aluminum detoxification. The study found that the CDC schedule results in the highest percentage of days an infant is in aluminum toxicity, reflecting chronic toxicity. The study introduced a new statistic: %alumTox, which measures the expected percentage of days (or weeks) an infant is in aluminum toxicity. Among the three schedules studied, the CDC schedule had the highest %alumTox[2].
Study 3: Impact of Catch-Up Vaccination on Aluminum Exposure
The third study by Lyons-Weiler et al. explored how catch-up vaccination impacts aluminum exposure due to new laws and post-social distancing. The COVID-19 pandemic placed significant stressors on the general public. Part of this included patients skipping well-child visits to reduce risk of exposure to SARS-CoV-2 virus. Published estimates of the duration of whole-body aluminum (Al) toxicity from vaccines in infants from birth to six months indicated that CDC’s recommended vaccination schedule leads to unacceptably long periods of time in which infants are in aluminum toxicity (as measured by %alumtox). We utilized established clearance and accumulation models to calculate expected per-body-weight whole-body toxicity of aluminum from vaccines considering for children of all ages under CDC’s catch-up schedule from birth to ten years, assuming social distancing for 6 months. Our updated pediatric dose limit (PDL) model assumes a linear improvement in renal function from birth to two years3.
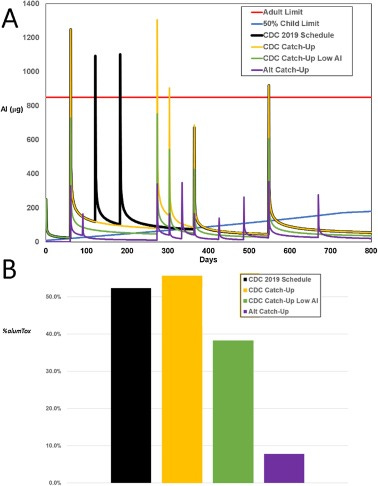
Our impact of the expected effects of CDC’s catch-up vaccination schedules, particularly in the context of the COVID-19 pandemic, was ahead of its time. The study utilized well-established clearance and accumulation models to calculate expected per-body-weight whole-body toxicity of aluminum. We urged caution in the mass re-starting of vaccination under CDC's Catch-Up schedule for children under 12 months. The study found that alternative spacing and use of non-aluminum containing vaccines could reduce whole-body toxicity and associated risks of morbidity[3].
Implications for Public Health Policy
The collective findings of these studies offer a more cautionary perspective on the safety of aluminum in pediatric vaccines. We called for a reevaluation of existing safety guidelines and advocate for more individualized vaccination schedules to minimize aluminum toxicity risks.
Future Directions
Given the global implications of these findings, there is an urgent need to extend this research to include comparative studies of aluminum toxicity due to vaccine schedules in different countries. Our ongoing efforts focus on a multi-disciplinary, international study that employs state-of-the-art computational models and real-world data.
Conclusion
The studies by Dr. Lyons-Weiler and colleagues at IPAK serve as a critical addition to the scientific literature on aluminum toxicity in vaccines. They highlight the need for a more nuanced approach to vaccine safety, one that takes into account individual variability and the cumulative effects of multiple vaccines.
Funding Appeal
These studies are 100% funded by you, the public. We appeal to you to invest in this crucial area of research, which has significant implications for public health policy and the well-being of future generations. The estimated budget for the proposed project is $25,000.
You can help support the meticulous work of Dr. Lyons-Weiler and his team, this progress report aims to serve as a cornerstone for securing funds for further studies in this vital area of public health research. The safety of our pediatric population, and by extension, the future of our society, hinges on the rigorous scientific evaluation of all aspects of vaccination, including the potential for aluminum toxicity.
Citations
[1]: Lyons-Weiler, J., & Ricketson, R. (2018). Reconsideration of the immunotherapeutic pediatric safe dose levels of aluminum. J Trace Elem Med Biol, 48, 67-73. [DOI: 10.1016/j.jtemb.2018.02.025](https://doi.org/10.1016/j.jtemb.2018.02.025)
[2]: McFarland, G., La Joie, E., Thomas, P., & Lyons-Weiler, J. (2020). Acute exposure and chronic retention of aluminum in three vaccine schedules and effects of genetic and environmental variation. J Trace Elem Med Biol, 58, 126444. [DOI: 10.1016/j.jtemb.2019.126444](https://doi.org/10.1016/j.jtemb.2019.126444)
[3]: Lyons-Weiler, J., McFarland, G., & La Joie, E. (2020). Impact of catch-up vaccination on aluminum exposure due to new laws and post social distancing. J Trace Elem Med Biol, 62, 126649. [DOI: 10.1016/j.jtemb.2020.126649](https://doi.org/10.1016/j.jtemb.2020.126649)

many years ago I lived in a tiny house in which the address was 35 Sunset Drive. While the sun did set every day it ws no surprise to me that it rose most days too. I too know that 35 plus 35 equals 70 plus a few more equals the number of childhood vaccines on the CDC schedule. I had no cows on my property nor did Satan ever come, but the CDC does have a lot of pigs. So without further contempletion, I can tell you there is no safe amount of aluminum you can inject into anyone, let alone an infant. I can also state that we don't know which children dump it or which hang onto aluminum. So, eliminate all childhood vaccines and by doing so you will eliminate all the aluminum you inject into them. For Satan's sake and for 666 or 999 I don't even buy aluminum foil.
Is it a coincidence that the word “vaccination” = 666 in English Gematria? Probably not.
If you look up the word “vaccination” in etymology you will find it is related to cows!!
And don’t the elite call us “useless cattle or chattle”?
vaccination (n.)
1800, used by British physician Edward Jenner (1749-1823) for the technique he publicized of preventing smallpox by injecting people with the similar but much milder cowpox virus (variolae vaccinae), from vaccine (adj.) "pertaining to cows, from cows" (1798), from Latin vaccinus "from cows," from vacca "cow," a word of uncertain origin. A mild case of cowpox rendered one immune thereafter to smallpox. "The use of the term for diseases other than smallpox is due to Pasteur" [OED].
Isn’t it strange that nowadays the vaccine schedule for children has multiplied many time since the 1970’s?
And all of a sudden children have all kinds of issues like “autism”, “asbergers”, “ADD”, “allergies” etc etc etc????
WOW what a coincidence huh?
I must be a “coincidence theorist!!!”
THEY LIE, THEY CHEAT, THEY STEAL, THEY HARM......because THEY are of the Devil!!!
Seek Jesus Christ NOW folks!!!
You WONT regret that decision!!!
Guaranteed!!!