


Lyons-Weiler: The Moratorium on Pathogenic Virus Gain-of-Function Research Must be Reinstated. HHS Commission Oversight Committee Proposed.
Regulation and "Surveillance" of GOF Research seem to be on the table. History has proven they are not enough. It's not a matter of if, but when. Let's fix regulatory capture while we're at it.

The original arguments for calling for a moratorium on gain-of-function research were made by a group of scientists and public health experts in 2014. The group of scientists and public health experts who made the call in 2014 included Dr. Marc Lipsitch, Dr. Richard Ebright, Dr. Bruce Alberts, and others.
They argued that such research posed an unnecessary risk to public health, as it could lead to the accidental release of potentially harmful organisms or the intentional misuse of these organisms by terrorists. The evidence used to win the argument included the potential for an accidentally released organism to cause an outbreak, as well as the fact that these organisms could be used in bioterrorism.
The lab escapes before 2014 that were cited by the group of scientists and public health experts who made the call for a moratorium in 2014 included the escape of H5N1 bird flu viruses from a lab in the Netherlands in 2011, the escape of a SARS virus from a lab in Germany in 2012, and the escape of H7N9 bird flu viruses from a lab in China in 2013.
But the public was not and is still not aware of the full extent of the history of biosafety laboratory failures. Here’s a short list from Wikipedia, starting in 1988. This is not a complete list of the known lab safety failures:
1988: Soviet Union. Marburg virus disease. Event: Laboratory-acquired infection.
1990: Soviet Union. Marburg virus disease. Event: Laboratory-acquired infection, death.
2001: United States. Anthrax. Event: Bioterrorism.
2002: United States. Fort Detrick. Anthrax. Event: containment breach.
2002: United States. West Nile virus. Event: Laboratory-acquired infection.
2003: Singapore. SARS-CoV-1. Event: Laboratory-acquired infection.
2003: Taipai. SARS-CoV-1. Event: Laboratory-acquired infection.
2004: Beijing. SARS-CoV-1. Event: laboratory infection, person-to-person transmission
2004: Russia. Ebola. Event: laboratory infection, death.
2004: United States (Plum Island): Foot-and-mouth disease virus. Event: Laboratory-acquired infection.
2005: US+17 other countries. H2N2 influenza virus. Event: testing kit distribution.
2005-2015: United States. Anthrax. Events. 74 shipments of live Anthrax (‘accidental’)
2007. United Kingdom Foot-and-mouth disease virus. Event: laboratory discharge.
2009. Germany. Ebola. Event: Laboratory-acquired infection.
2009. United States. Yersinia pestis. Event: Laboratory-acquired infection, death.
2010. United States. Swine Fever Virus. Laboratory accidental release.
2010. United States. Cowpox. Laboratory-acquired infection.
2011. Australia. Dengue. Laboratory-acquired infection.
2012. United Kingdom. Anthrax. Accidental shipments of live virus.
2012. United States. Neisseria bacterium. Laboratory-acquired infection. Death.
2013. United States. H5N1 Influenza virus. Laboratory-acquired infection.
2014. United States. H1N1 Influenza virus. Laboratory animal escape.
2014. United States. H5N1 influenza virus. Accidental shipment (CDC to USDA).
2014. United States. Smallpox. Event: Laboratory mislabelling (last samples had been thought to be destroyed).
2014. United States. Burkholderia bacterium. Outdoor animal facility infection.
2014. Sierra Leone. Ebola. Event: Laboratory infection.
2014. South Korea. Dengue. Laboratory infection.
2016. United States. Zika. Laboratory infection.
2016. Australia. Nocardia bacterium. Laboratory infection.
2018. Hungary. Ebola. Event: Laboratory infection.
2019. France. Prions. Laboratory infection ten years prior. Death.
2019. China. Brucella. Infection.
2021. Taiwan. SARS-CoV-2 (Delta). Laboratory leak.
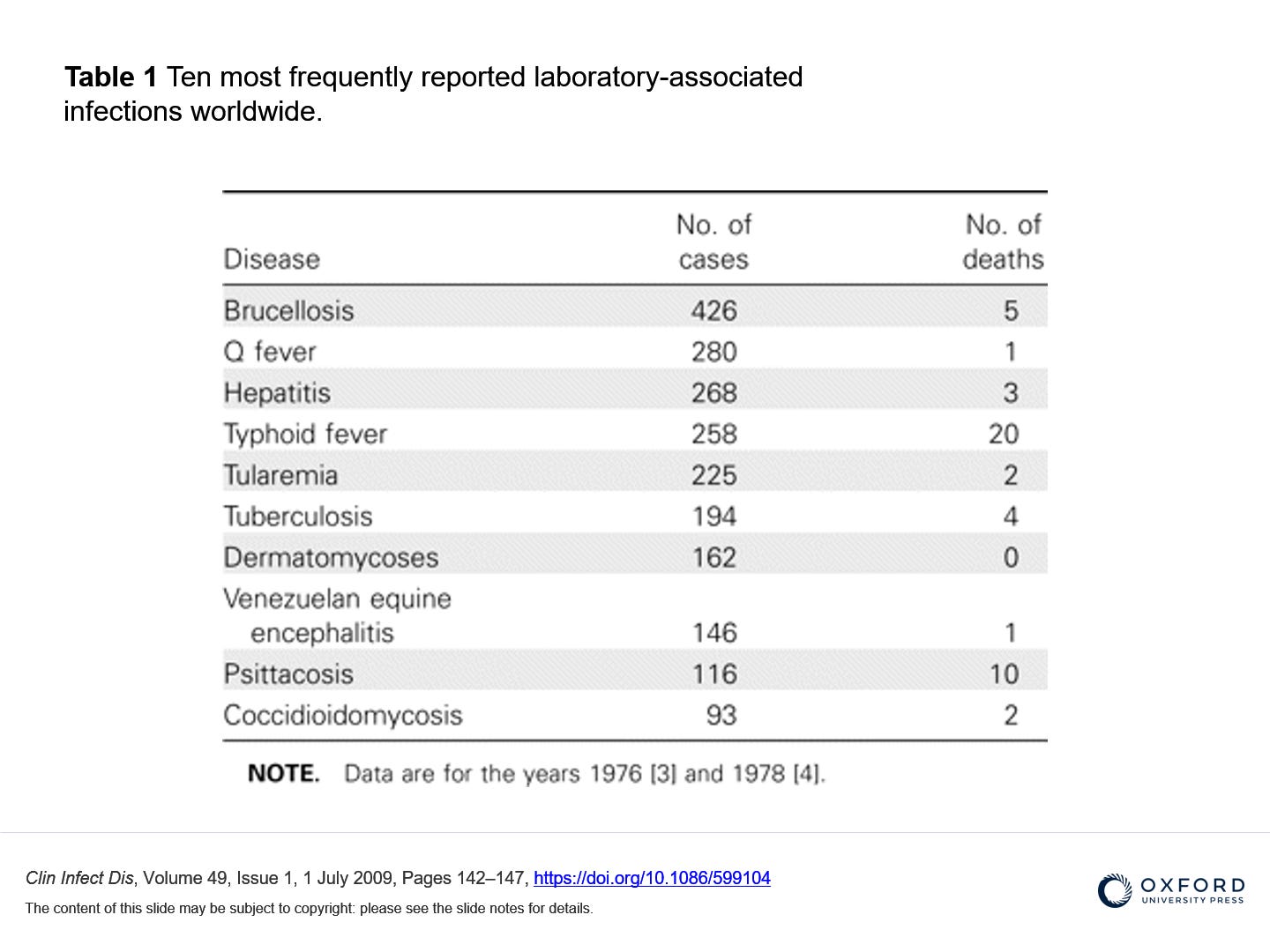
A review of laboratory-acquired infections published in 2009 shows far more such incidents (images © 2009 by the Infectious Diseases Society of America):

Those who successfully argued against the moratorium argued that the research was necessary to better understand infectious diseases and to develop countermeasures against them. However, they ultimately lost the argument due to the perceived risks posed by the research outweighing the potential benefits.
Even given the release of the SARS-CoV-2 virus on the world’s population, and following the devastating consequences, then-NIAID Director Anthony Fauci argued that the benefit from such research outweighed the risk even if another pandemic took place. One of the original members of the group calling for the original moratorium - Dr. Richard Ebright - places the blame squarely on Fauci for “thwarting” attempts to regulate GOF research. From Counterpunch.org:
“What went wrong for the Cambridge Working Group thesis during the 2014-2016 USA official moratorium and deliberative process on Gain-of-Function Research of Concern (GoFRoC)?
The Director of the National Institute of Allergy and Infectious Diseases (NIAID) and the Director of the National Institutes of Health (NIH) have systematically thwarted efforts by the White House, Congress, scientists, and science policy specialists to regulate GoF research of concern and even to require risk-benefit review for projects involving GoF research of concern.
In 2014, the Obama White House implemented a “Pause” in federal funding for GoF research of concern. However, the document announcing the Pause stated in a footnote that: “An exception from pause may be obtained if head of funding agency determines research is urgently necessary to protect public health or national security”. Unfortunately, the NIAID Director and the NIH Director exploited this loophole to issue exemptions to projects subject to the Pause –preposterously asserting the exempted research was “urgently necessary to protect public health or national security”– thereby nullifying the Pause.
In 2017, the Trump Administration announced a Potential Pandemic Pathogens Control and Oversight (P3CO) Framework that implemented a requirement for risk-benefit review of GoF research of concern. However, the P3CO Framework relies on the funding agency to flag and forward proposals for risk-benefit review. Unfortunately, the NIAID Director and the NIH Director have declined to flag and forward proposals for risk-benefit review, thereby nullifying the P3CO Framework.”
Read the full interview:How Anthony Fauci "Systematically Thwarted" the Pause in US Gain-of-Function Research: an Interview with Dr. Richard H. Ebright - CounterPunch.org
Related: EXCLUSIVE: Controversial experiments that could make bird flu more risky poised to resume
Now, Pfizer Board member Scott Gottlieb, who used his profile as former FDA Commissioner to promote Pfizer’s mRNA vaccine, has called for more regulations on “high-risk research”, under the “assumption there’s a ‘probability’ COVID (sic: the SARS-CoV-2 virus) originated from a lab leak.
Face The Nation’s Twitter post-spot-lighting their interview of Gottlieb is peppered with comments critical of Face The Nation for their softball questions.

Gottlieb also says that we should “talk” about whether we’re going “outlaw” this type of research, that it’s “time to get serious”, and, remarkably, that the worst labs around the world get the riskiest research because they are willing to do it, and calls for “surveillance” over these projects, which he claims have “no commercial value” and are only justified by “national security interests”.
Pfizer, Gottlieb’s employer, has reaped billions in investment revenue stemming from projections of 15 to 30 billion in profits from SARS-CoV-2 vaccines (Source: The Guardian).
Where was Gottlieb during the first (Jan 30, 2020), second, and third go-round on the laboratory origins of SARS-CoV-2?
And where is he now on the abject failure of Pfizer’s product?
Why is CBS News not holding Pfizer accountable for the adverse events, deaths, and uptick in all-cause mortality that has followed the release of their product on an unwitting and trusting public?
HHS Citizens Oversight Commission Needed
We must have an independent citizen’s commission that directs HHS - and that reports to but does not answer to - the President of the United States. This Commission must be able to fire Directors (and any other employees) of any of the three-letter agencies for not following the charter of the agency allowed by Congress, for violating the law, and for acting against the interests of the people of the United States of America. The Commission members and their family members must not have any conflicts of interest and must swear an oath to Congress to never receive funding, favors, or services in return for their votes or positions on regulating the agencies. They must not be otherwise currently elected to or appointed to any branch of the Federal government. They must also serve with term limits and new members should be appointed by retiring Commission members. Their membership should be approved by a bipartisan panel of Congress. The Commission should have line-item veto power over the agency’s budgets - and they should have the power to terminate specific projects and project areas. They should be able to direct agency heads on their priorities for action: research direction, mitigation, policy enforcement, and day-to-day management practices.
If any member is found to have acted inappropriately due to influence from corporations regulated by any HHS agency, or foreign entities, the Commissioner would be subject to jail time for lying to Congress in their oath.
There should be no chairperson, and the Commission should have an odd number of members to prevent stalemates on decisions.
See Also
Hhs needs to be split up decentralized distributed accross states and shrunk to less than 1 quarter of what they are now.
A nation of sheep will beget a government of wolves. Edward R. Murrow