


Genetic Variation Across Human Populations Influences SARS-COV-2 Binding Capacity for ACE2 Receptors
Once again, Mr. Kennedy has made a fool of CNN and mainstream media for not even bothering to investigate the basis of his comments.

Just in case anyone like CNN was wondering: Host susceptibility to COVID-19 varies with genetics and ethnicity usually correlates with genetics. The host susceptibility variation is based on differences in ACE2 receptors.
Hu P, Bauer VL, Sawyer SL, Diaz-Griffero F. Human ACE2 Polymorphisms from Different Human Populations Modulate SARS-CoV-2 Infection. Viruses. 2022 Jun 30;14(7):1451. doi: 10.3390/v14071451. PMID: 35891433; PMCID: PMC9319759.
The COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in over 6 million deaths worldwide. The high variability in COVID-19 symptoms remains one of the most interesting mysteries of the pandemic. Genetic and environmental factors are likely to be key determinants of COVID-19 symptomatology. Here, we explored ACE2 as a genetic determinant for SARS-CoV-2 infection and COVID-19 symptomatology. Each human genome encodes two alleles of ACE2, which encodes the cell entry receptor for SARS-CoV-2. Here, we determined whether naturally occurring human ACE2 (hACE2) polymorphisms in the human population affect SARS-CoV-2 infection and the severity of COVID-19 symptoms. ACE2 variants S19P, I21V, E23K, K26R, K31R, N33I, H34R, E35K, and T92I showed increased virus infection compared to wild-type ACE2; thus, these variants could increase the risk for COVID-19. In contrast, variants D38V, Y83H, I468V, and N638S showed reduced infection, indicating a potential protective effect. hACE2 variants K26R and T92I increased infection by three-fold without changing the levels of ACE2 on the surface of the cells, suggesting that these variants may increase the risk of severe COVID-19. On the contrary, hACE2 variants D38V and Y83H decreased SARS-CoV-2 infection by four- and ten-fold, respectively, without changing surface expression, suggesting that these variants may protect against severe COVID-19. Remarkably, all protective hACE2 Polymorphisms were found almost exclusively in Asian populations, which may provide a partial explanation for the low COVID-19 mortality rates in Asian countries. Thus, hACE2 polymorphisms may modulate susceptibility to SARS-CoV-2 in the host and partially account for the differences in severity of COVID-19 among different ethnic groups.
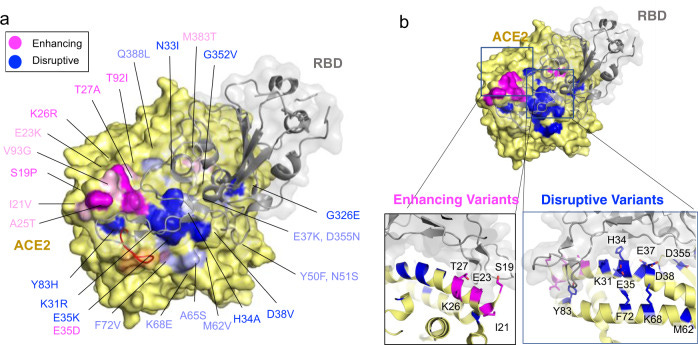
COVID-19 is a respiratory illness caused by a novel coronavirus called SARS-CoV-2. The viral spike (S) protein engages the human angiotensin-converting enzyme 2 (ACE2) receptor to invade host cells with ~10–15-fold higher affinity compared to SARS-CoV S-protein, making it highly infectious. Here, we assessed if ACE2 polymorphisms can alter host susceptibility to SARS-CoV-2 by affecting this interaction. We analyzed over 290,000 samples representing >400 population groups from public genomic datasets and identified multiple ACE2 protein-altering variants. Using reported structural data, we identified natural ACE2 variants that could potentially affect virus–host interaction and thereby alter host susceptibility. These include variants S19P, I21V, E23K, K26R, T27A, N64K, T92I, Q102P and H378R that were predicted to increase susceptibility, while variants K31R, N33I, H34R, E35K, E37K, D38V, Y50F, N51S, M62V, K68E, F72V, Y83H, G326E, G352V, D355N, Q388L and D509Y were predicted to be protective variants that show decreased binding to S-protein. Using biochemical assays, we confirmed that K31R and E37K had decreased affinity, and K26R and T92I variants showed increased affinity for S-protein when compared to wildtype ACE2. Consistent with this, soluble ACE2 K26R and T92I were more effective in blocking entry of S-protein pseudotyped virus suggesting that ACE2 variants can modulate susceptibility to SARS-CoV-2.
Had this argument just this Sunday at a gathering of friends and of course politics came up and I suggested only person I know that I would support and was Robert F Kennedy Jr and they all started laughing and one guy next to me said no I can’t what he said about the Jews I asked him what did he say about the Jews then spouted the article in the ny post said I said it’s false absolutely false I told him what he really did say and can send them the literature and thePubMed citation article on the genetics ofthe Covid to19 virus this is why this is important I’m bringing this up because Robert F Kennedy Dr Was on top of this smear campaign came right out and I got an email about it and I looked into it and I posted it on my Facebook but if I didn’t I don’t read the NY post I wouldn’t have any argument ammunition to counter what was said because I wouldn’t know anything about the statement that is why it’s key that NOT only Kennedy has great information but know what your opposition is saying so you can refute it in the timing proper manner Destruct their argument so we are going to be the soldiers on the front line because you’re not gonna hear much of it in the mass media except for smearing him a and vilifying him so kudos to John F. Kennedy Jr to be on top of it and posting it to his followers
I can't believe it's taken this long (4+ yrs) for this to get mentioned publically🤦♀️🤦♀️🤦♀️🤦♀️