


Answer to: 24-hr Quiz on the Safety Estimates of Vaccine Boosters
Many brave souls tried to provide an estimate to this first Popular Rationalism 4-hr quiz. Let's break it down.

Yesterday, I posted the first Popular Rationalism 24-hr quiz, which you can read here.
Many brave souls tried to provide an estimate of the rate of Serious Adverse Events (SAEs) in a booster dose when 10.1% of the individuals in the study group reported SAEs or died when they received the first dose. Some said it could not be answered due to insufficient information.
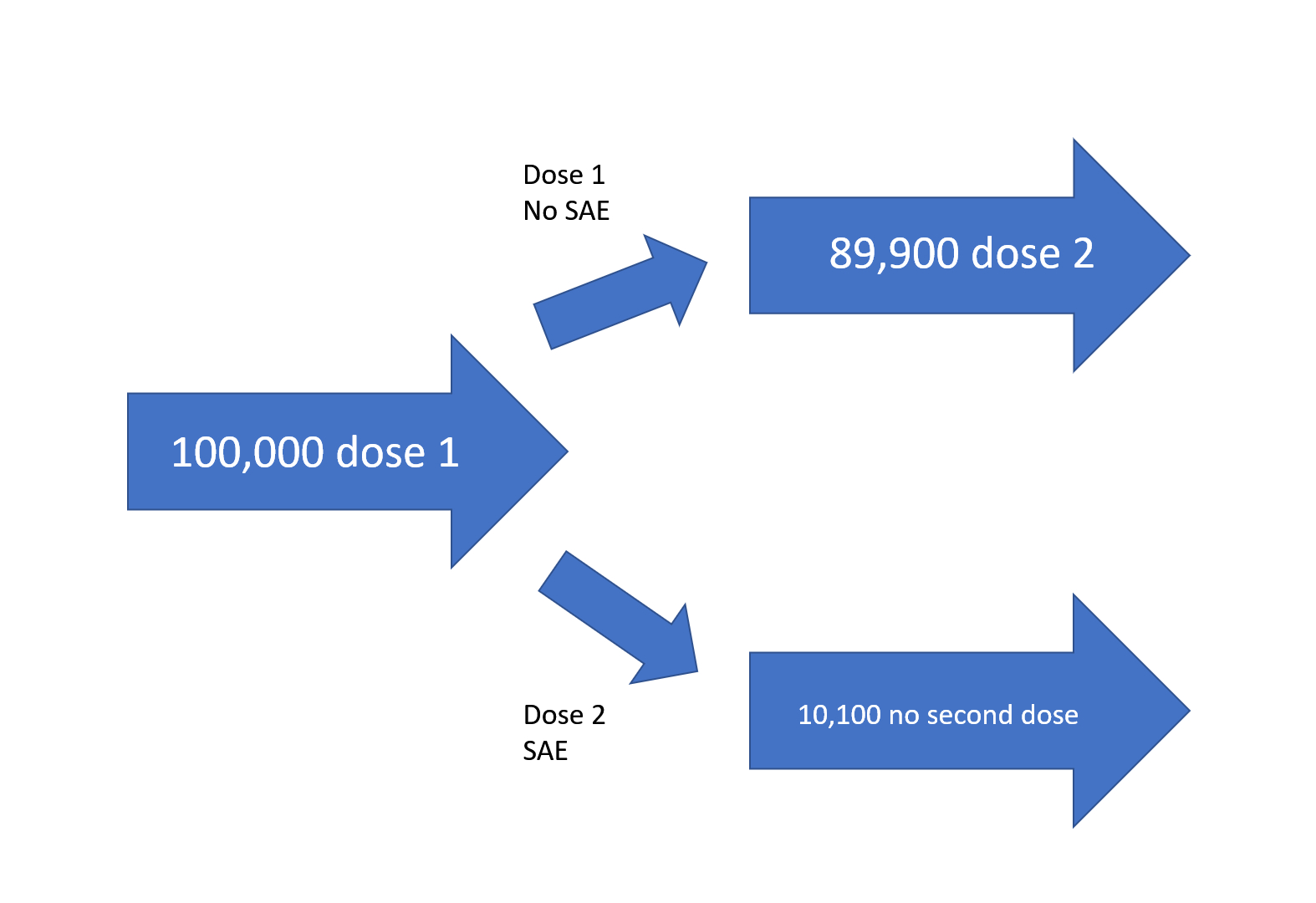
The question was posed with a 100,000 starting group, of which 89,900 experienced neither an SAE nor died due to the first dose:
“The Vaccinologist View
First exposure: N=100,000
Drop-out or reported SAE: 10,100
Reported SAE rate (if unbiased): 10.1%
Second exposure: N=100,00-10,100 = 89,900
24-HR QUIZ QUESTION: What will the unbiased SAE population rate be for the booster in the second exposure?”
The answer:
It is impossible to estimate the population rate of SAEs for the booster because, in the ethical execution of clinical trials, people are left out of the second dose if they experience an SAE (clearly so if they die due to the first dose!), but in real-world settings, people who experience an SAE are still pressured to accept a booster, and SAEs are denied to have occurred and are not taken seriously by doctors.
Explanation
In the first leg of the study, we started with 100,000 people in our sample. In the second leg, we’re down to 89,900 (as made clear “Second exposure: N=100,00-10,100 = 89,900” because 10.1% of the people in the trial could not tolerate the vaccine.
The people who left the study were susceptible to harm from the vaccine’s first dose, while the people who stayed in the study were (ostensibly) safe from immediate harm from the first dose.
We can expect in the clinical trial setting that a higher percentage of the 89,900 will be able to tolerate the booster (second dose) because they did not experience an SAE in the first leg.(1see caveat, below). That group is said to be enriched for vaccine-tolerant individuals.
This is called SURVIVOR BIAS (aka “Survival Bias” or “Survivorship Bias”), and is a well-known problem with clinical trials that require second, or third exposures.
We’ve seen this in other Popular Rationalism articles
The problem is that we cannot calculate an estimate of the SAEs for the general population from the clinical trial setting unless everyone in the trial was forced to receive two doses, which would be highly unethical, and impossible if anyone died.
This problem is a problem in the study of all vaccines that involve boosters, and is a form of translational failure (failure to derive an accurate, unbiased estimate of what is expected to occur in the whole population (e.g., the US population), from a study sample (e.g., our 100,000).
Although it’s true that one cannot expect that the SAE rate in Sample 2 will be estimable from that from Sample 1, the problem is not merely that Sample 1 and Sample 2 are not the same.

Due to this fact, Sample 2 - those who received both doses - is not representative of the general population, and yet CDC and FDA’s recommendations - and certainly mandates - actively work to make sure that the world thinks the risk to the entire population is represented by the risk of Sample 2. This is evidenced by the persecution of physicians who give medical exemptions in states where medical exemptions are allowed, and in the persecution of physicians who abide by informed consent and patient choice.
There is no point in going through clinical trials and observational studies of multi-dose (“booster”) vaccines unless the entire set of outcomes of the trials is then translated into clinical practice. Otherwise, the medical community is basing their risk assessment only on the data from people who had no SAEs in the first dose.
There was one outcome that was acknowledged as problematic: anaphylaxis. The others are ignored. People who are offered the second dose of COVID-19 vaccines are not asked “did you have any bleeding problems?” “did you have a problem with blood clots” or “did you experience neurological problems” or “did you experience any problems with your heart” after the first dose? Further, those rare people who have gone on to receive three doses are not asked the same after the second dose. Instead, when they bring up these established side effects, some of the physicians tell them “those were not due to the vaccine”. Instead, the vaccination program has had to face the stark and hard reality that Americans do not want the vaccine every 4 months, or, likely, every year.
Here are some references for other examples of survivor bias to expand your knowledge. The third study listed, Survival bias in observational studies of the impact of routine immunizations on childhood survival, by Peter Aaby et al. is especially eyebrow-raising.
Want more information like this? You can enroll in “The Math of Vaccine Science” (click on the link or image below) with a tenured epidemiologist @ IPAK-EDU where these types of details will be made clear for a wide number of types of calculations and estimations used in vaccine studies.
References
Survivor Treatment Selection Bias and Outcomes Research https://www.ahajournals.org/doi/10.1161/circoutcomes.109.857938
Survivor treatment selection bias in observational studies: examples from the AIDS literature https://pubmed.ncbi.nlm.nih.gov/8624068/
Survival bias in observational studies of the impact of routine immunizations on childhood survival
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-3156.2006.01773.x
I want to thank everyone who participated in this first 24-hr quiz by leaving their estimates in the comments. Lest anyone think it was a “trick question”, it was not: the answer is the answer. Watch for more 24-hr quiz challenges on Popular Rationalism!

This assumes that the risk of an autoimmune-related SAE is not made higher by a second exposure due to pathogenic priming (repeated exposure to a foreign antigen source that leads to autoimmunity). See Pubmed for papers related to Pathogenic Priming.
Logically Survivor bias makes sense, but I know that before your discussion and helpful sample showing the breakdown, I had no real idea.
I doubt 99% of practicing medical professionals are aware of the concept, and of how this sleight of hand makes all of the study data more than suspect.
The CDC and FDA scientists understood this concept of Survivor bias and the way it impacts understanding of product safety in drug trials.
Even well read science geeks like myself are playing catch-up, and can’t realistically know as much as a person with a doctorate in Epidemiology.
This makes it all the more egregious that our government’s scientific community isn’t breaking ranks en mass for such extreme dishonesty in how the EUA of the Covid-19 shots were approved and mandated.
We pay their salaries. We are entitled to their honesty.
Interesting problem. The study population changed when death forced the dry tinder out of the study. I don't see any way to adjust the data to adjust for the bias.
"This is called SURVIVOR BIAS (aka “Survival Bias” or “Survivorship Bias”), and is a well-known problem with clinical trials that require second, or third exposures. "
I saw a study where the same people were used in the vaccinated and unvaccinated groups. All started out in the unvaccinated group and were vaccinated over time. There was clear survivorship bias in that study.