

Yet Another Final, Respectful Response to Virus Denialism.
Tom addressed some, well one of my points that show that their paradigm is falsified by data. Here is my response to his failed rebuttal video.

Virus denialists have a large following. Tom Cowan, in particular, believes that we need to be able to use our own senses to know something exists. This is a simplifying but empirically impoverished viewpoint on what we can know via Science.
Tom took to Bitchute in a video to respond to eight points that I posted on the matter.
He did not address eight points. Here, without adding to disunity, I rebut (again, and likely for the last time), the claims by providing scientific evidence.
An Aside
As an aside, understand that I am reluctantly taking my time to write this article, because I know that those promulgating virus denialism will not pay heed to any scientific evidence I provide that demonstrates the falseness of their claims.
When I have debated virus deniers in the past and provided references to studies that directly rebut their false claims, they have ignored the scientific evidence I provided and continued to make the same statements - the very next day. I know this because after I debated a virus denier in a recorded debate, I happened to also be in a zoom meeting the next day with one of the participants in the event. They acted as if the studies I sent to them did not exist and simply repeated the same faulty claims that were made by my opponent the day before.
In his Bitchute, it is interesting that Tom skipped over my Point #1: that Koch himself failed, using his own criteria, to identify now-known pathogens. This is a rather important point, and Tom's failure to address it speaks volumes.
In my response, I will simply provide studies that show that the specific claims about SARS-CoV-2 virus by virus deniers like Cowan are factually incorrect. The studies I show are representative of a much, much larger body of published science that shows the basic claims being made are false.
I will not speculate on the motivation of those who would care to continue to ignore studies. They themselves can address that obvious question.
Koch’s Postulates
Koch developed rules to follow by which one can determine if a pathogen is responsible for a disease. The reader should be aware these were published in 1884; Koch updated them to relax the first postulate when he discovered asymptomatic transmission. Also, Koch’s postulates fail to apply to typhoid fever, diphtheria, leprosy, relapsing fever, and Asiatic cholera specifically because it is difficult to create ‘the disease anew’ in animals upon infection (Ref).
Koch’s postulates were addressed head-on for the SARS virus in 2003. See
Koch's postulates fulfilled for SARS virus.
As originally written, Koch’s four criteria were:
(1) The microorganism must be found in diseased but not healthy individuals;
We know that asymptomatic COVID-19 infection can occur. Koch himself had to modify his postulates after he discovered asymptomatic infections could occur.
(2) The microorganism must be cultured from the diseased individual;
SARS-CoV-2 has, in fact, been cultured. It’s a matter of routine:
Wurtz N, Penant G, Jardot P, Duclos N, La Scola B. Culture of SARS-CoV-2 in a panel of laboratory cell lines, permissivity, and differences in growth profile. Eur J Clin Microbiol Infect Dis. 2021 Mar;40(3):477-484. doi: 10.1007/s10096-020-04106-0.
“In the present work, we tested 4 strains of SARS-CoV-2 locally isolated on a panel of 34 cell lines present in our laboratory and commonly used for the isolation of human pathogenic microorganism. After inoculation, cells were observed for cytopathic effects and quantitative real-time polymerase reaction was used to measure the virus replication on the cells. We were able to obtain growth on 7 cell lines, 6 simian, and the human Caco-2. The cytopathogenic effects are variable, ranging from lysis of the cell monolayer in 48–72 h to no cytopathic effect in spite of intense multiplication, as in Caco-2 cells. Interestingly, effect and multiplication varied widely according to the strain tested.”
Sung A, Bailey AL, Stewart HB, McDonald D, Wallace MA, Peacock K, Miller C, Reske KA, O'Neil CA, Fraser VJ, Diamond MS, Burnham CD, Babcock HM, Kwon JH. Isolation of SARS-CoV-2 in Viral Cell Culture in Immunocompromised Patients With Persistently Positive RT-PCR Results. Front Cell Infect Microbiol. 2022 Feb 2;12:804175. doi: 10.3389/fcimb.2022.804175.
“Viral RNA and cultivable virus were recovered from the cultured cells after qRT-PCR and plaque assays. Of 20 patients, 10 (50%) had a solid organ transplant and 5 (25%) had a hematologic malignancy. For most patients, RT-PCR Ct values increased over time. There were 2 patients with positive viral cell cultures; one patient had chronic lymphocytic leukemia treated with venetoclax and obinutuzumab who had a low viral titer of 27 PFU/mL.”
Even the important study showing that use of too high RT-PCR cycle thresholds led to false positives used the ability to create a culture and infectiousness from clinical samples
Singanayagam A, Patel M, Charlett A, Lopez Bernal J, Saliba V, Ellis J, Ladhani S, Zambon M, Gopal R. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill. 2020 Aug;25(32):2001483. doi: 10.2807/1560-7917.ES.2020.25.32.2001483.
(3) Inoculation of a healthy individual with the cultured microorganism must recapitulated the disease;
There are far too many studies that show that animals infected with the virus get sick, and that natural immunity is protective:
K18-hACE2 mice develop respiratory disease resembling severe COVID-19 https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1009195
Primary exposure to SARS-CoV-2 protects against reinfection in rhesus macaques - https://www.science.org/doi/10.1126/science.abc5343
Intranasal exposure of African green monkeys to SARS-CoV-2 results in acute phase pneumonia with shedding and lung injury still present in the early convalescence phase https://virologyj.biomedcentral.com/articles/10.1186/s12985-020-01396-w
Experimental infection of domestic dogs and cats with SARS-CoV-2: Pathogenesis, transmission, and response to reexposure in cats https://www.pnas.org/doi/10.1073/pnas.2013102117
For obvious ethical reasons, we will never see the experimental infection of healthy individual humans with the SARS-CoV-2 virus. However, the Singanayagam et al. study examined the infectiousness of samples from clinical samples:
“The RT-PCR cycle threshold (Ct) values as a measure of SARS-CoV-2 viral load showed that the level of SARS-CoV-2 RNA in the Upper Respiratory tract was greatest around symptom onset, steadily decreased during the first 10 days after illness onset and then plateaued.
In days −2 to 7 since symptom onset geometric mean (GM) Ct was 28 (95% CI 27.8 to 28.6).
In the second week (days 8 to 14), GM Ct was 31 (95% CI: 9.8 to 32; p < 0.001 compared with week 1)
After 14 days, GM Ct was 32 (95% CI: 31.6–34.5; p = 0.01 compared with week 1 (there was no significant difference in Ct values between days 8–14 and after 14 days).
Cultivable virus was isolated from 133 (41%) samples (from 111 cases).
Detection of cultivable virus peaked around the time of symptom onset.
In the 246 samples from 176 symptomatic cases where the date of symptom onset was known, 103 (42%) from 81 cases were culture positive Implying that 30 samples from which the virus was cultured, were asymptomatic.
Median Ct of all 324 samples was 31 (interquartile range (IQR): 27.5–33.9; range: 17.5–41.8). 233 cases (92%) were classified as non-severe (asymptomatic or mild-to-moderate) and 20 (8%) had severe illness (requiring intensive care admission and/or fatal).
There was no difference in Ct values between those with asymptomatic (median Ct = 31; IQR: 28–33), mild-to-moderate (median Ct = 31; IQR: 27–35) or severe (median Ct = 33; IQR 28.–34) illness (p = 0.79).
A stratified comparison of the severe cases over time showed a similar result.
Ct values were lower in week 1 than week 2. There was no difference in culture positivity rate from 62 samples of 61 asymptomatic cases: 21 of 62 samples from asymptomatic individuals vs 112 of 262 samples from symptomatic individuals (estimated odds ratio (OR) = 0.66; 95% CI: 0.34–1.31.
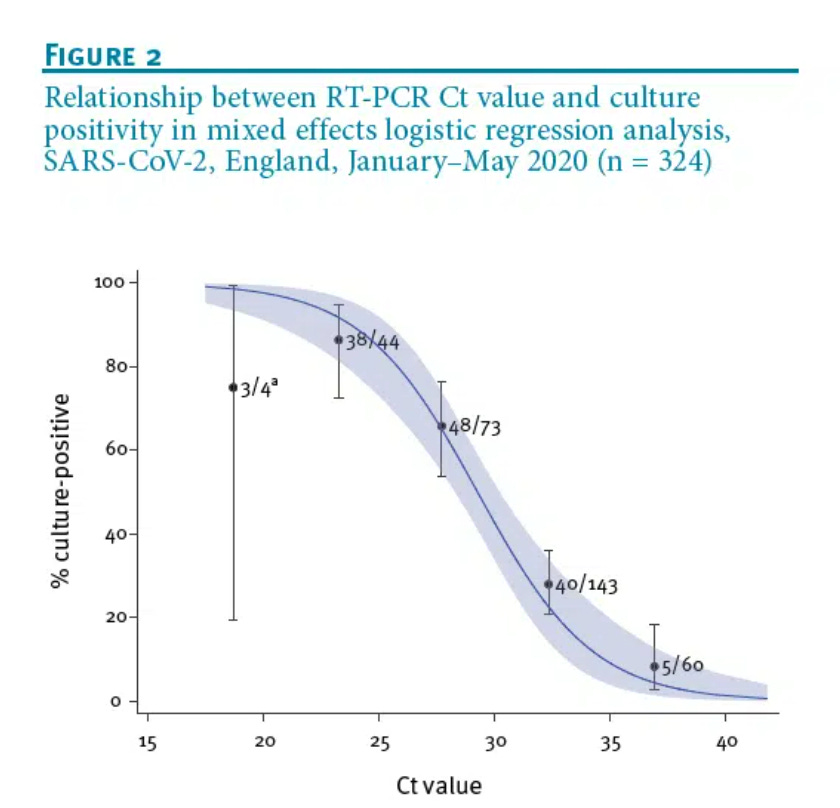
Similar to Bullard and colleagues’ and Piralla’s findings there was a strong relationship between Ct value and ability to recover infectious virus. The estimated OR of recovering infectious virus decreased by 0.67 for each unit increase in Ct value (95% CI: 0.58–0.77).
Virus propagation was successful from 5/60 samples with Ct > 35; all five were from symptomatic cases and none had severe illness. The estimated probability of recovery of virus from samples with Ct > 35 was 8% (95% CI: 2.8%–18%).”
(4) The microorganism must be re-isolated from the inoculated, diseased individual and matched to the original microorganism.
The studies above in fact satisfy this criterion as well, however this study actually examined the evolution of the SARS-CoV-2 virus in individual, infected animals (this means that we are far beyond the more than elementary ‘matching’ phase; the sequences are compared to each other as matter of routine.
Evidence Beyond Koch’s Postulates
The comparison of the pathogenicity of the pathogen going into an organism and going out is not expected to be identical; in vivo replication (https://pubmed.ncbi.nlm.nih.gov/35062281/), serial passage (Ref), and enculturation in “pure culture” (Ref) are expected to lead to changes in the virus via evolution.
This does not mean the basics have not been satisfied. It just means Koch’s Postulates limit cognition to basics, whereas the additional, more advanced knowledge - that could not exist unless the virus exists - is not taken into consideration.
It’s 2022, not 1884; the evolution of the virus itself within specific individuals has been studied - going far, far, far beyond Koch’s postulates.
Reminder that the basics have been satisfied, over and over and over
"To represent COVID-19 in our evolutionary cousins, the researchers infected 8 monkeys with SARS-CoV-2 via nose, trachea, eyes and/or mouth, and studied them for 3 weeks." https://www.novusbio.com/antibody-news/understanding-covid-19-through-sars-cov-2-infected-monkey-model
Why This Really Matters
The reality is that fighting against the totalitarian oligarchy with virus denialism is like binding one's own hands behind one's back after gagging yourself. As a virus denialist, you instantly delegitmize every other point that you would like to make among those people who know that viruses exist - including arguing that natural infection is superior, that the RT-PCR testing approach is fatally flawed, and even arguing that early treatments work.
Cowan claims that he has been consistent, and denies moving the goal poast, and yet now his current measure of evidence needed to believe that the virus exists is that one must be able to see it with the naked eye (he says so in his video).
We do not rely exclusively on our own senses to be able to accept things we can measure via technology.
You can't see Pluto with the naked eye. Yet you can use a telescope or a powerful pair of binoculars and see the planetoid. For scientists, the sequences derived are analyzed and assembled (not “generated”) using chemical reactions and computer algorithms. It is theoretically possible for a human being to create an alignment from the millions of reads that are produced via next-generation sequencing, but it would take too long. The sequencers and the sequence alignment algorithms are the microscopes of our generation.
Tom Thinks Bacteriophages are Catabolic Products of Stressed-Out Bacteria
According to Tom, when you stress a bacterium, the bacteria “break down” and they “turns into bacteriophages”. That is absurdly incorrect. Bacteriophages are duplodnaviria viruses that infect and replicates within bacteria and archaea.
Here’s a photograph of a bacteriophage for those who might like to “see” one:

Source: https://textbookofbacteriology.net/phage.html
Again, bacteriophages are viruses.
So, as convincing as Tom Cowan and other virus deniers may seem to be:
No, my points are not “epidemiology”.
Yes, the virus has been isolated and visualized.
Yes, the viral protein structures have been determined using X-ray crystallography.
Yes, viral evolution has been studied in detail.
No, the nucleotide sequence data have not been "generated" by computer.
Yes, the virus has been used to make animals sick.
Yes, samples from sick animals have been transferred to healthy animals and the newly infected animals made sick.
For those interested, Hammond denies calling Tom a "Cancer".
Because the deniers refused to accept the evidence right in front of them, this is the last time I will communicate studies to help virus deniers face the facts. I won’t be replying (and will not reply) to comments to my substack articles that imply “this entire article is pointless because the virus does not exist”. We need to focus on real problems and real issues. There is science to be done, rights to be protected and preserved, early therapies to promote, courses to be taught, and without being disrespectful, I simply do not have time to constantly address this.
First of all, to call it "denialism" is not just an insult but it's wrong...nobody investigating the virus is in denial. We have come up with findings that all involve the use of metagenomics to construct the "virus" and/or the use of in silico, theoretical "sequences." I'm not sure how to get past this paywall-style refusal to allow that discussion. To swat people and say they are denialists has gone beyond a mere error and entered the realm of sheer intellectual dishonesty.
Those who know me know that my task and quest as a journalist was to understand the SCOV-2 PCR assay. And nearly three years in, my questions are: if there is whole live virion from a human host, why wasn't that sequenced and instead, these metagenomic things have been used? Also, why are they using metagenomics for ALL of these "sequences" and not doing denovo from uncontaminated samples of BALF? Why do we need calf and monkey cells added to the genetic broth?
Second, if there is a real sequence, why are the primers for all PCRs ALL in silico?
Third, why does CDC use terms like "mimicked clinical specimen" and "contrived virus"? That needs to be accounted for.
Finally, we have 209 responses from governments and institutions in 35 countries saying they have no evidence of a sample of whole SARS-CoV-2 taken from a human host
It would seem to be that the only people in denial are pretending that this set of conditions leads to the conclusion that somebody actually has a sample of this stuff said to have killed seven million people and responsible for the shutdown of the economy and the destruction of the modern world.
Thank you for taking this head on. I talk about this is in all of my presentations. We have electron microscope images of these viral particles outside human cells, inside human cells, and attached to human cells. We understand the biological mechanisms whereby they are pulled into cells, copied, and released. The problem is, we have never actually seen one do that, and we never will due to the limitations of microscopy.