


What Would Happen if the PCR Test Were Disproven?
We have an IRB Proposal to sequence clinical samples and disprove the bogus PCR tests. All we need now is funding. That's up to you.

A blog article from 10/2020 was an early rational voice on False Positives. We are about to suffer badly due to OSHA's testing requirements due to work loss.
See: What tests to use, when, why—and why not? Pitfalls of mass testing for COVID-19
The article shows that when the prevalence of a disease is low, the % of positive results that are false explodes:
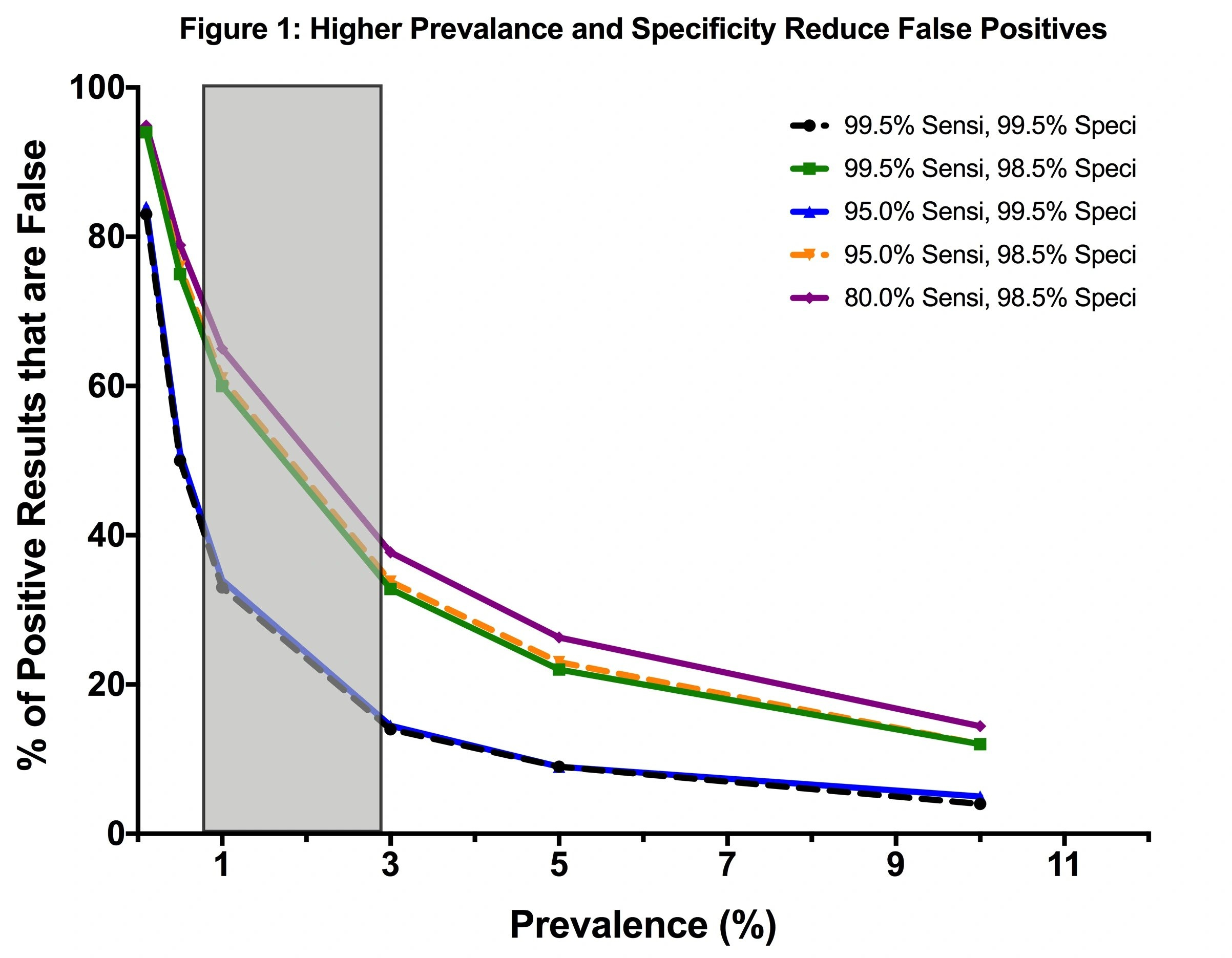
The prevalence of a disease is how many people are currently infected - a statistic avoided by public health data depots from the beginning.
It’s been known, well, forever, in clinical diagnostics that if you screen for a condition, including infections, using tests that have false positives - positive results from patients that do not have the infection - you’ll end up with more false positive results than true positive results when the prevalence is low.
By all measures, SARS-CoV-2 prevalence is low.
I warned about this in March 2020. Others have as well. Dr. Sin Hang Lee has pointed to a result in a Pfizer SARS-CoV-2 clinical trial that leads to an estimate of 91% false positives among all positives. His own sequencing study showed 30% false positives - and 40% false negatives - in a collection of reference sample sets sent to him that were labeled using RT-PCR as the “gold standard”. In fact, FDA’s website considers sequencing of parts of a virus as the gold standard - not PCR.
Other published estimates are available (Basile et al.)
(See: Accuracy amidst ambiguity: false positive SARS-CoV-2 nucleic acid tests when COVID-19 prevalence is low) and others I’ve cited many times in many places.
I warned early on that the risk of false positives could be devastating on my podcast #UnbreakingScience. They contributed to the lockdown, and the lockdown is known to have had no net desired effect on the spread of COVID-19.
Others are now waking up to the costs of the false positives.
See 2021 - The impact of false positive COVID-19 results in an area of low prevalence
The list the consequences of false positive results in this setting can have several adverse effects. These include:
“unnecessary treatment and investigation
missing or delayed surgery
unnecessary isolation and contact tracing with subsequent negative impact on workforce and resources
a risk of subsequent increased exposure if the individual changes their behaviour as a result of believing that they have been infected
the individual being placed with other inpatients with COVID-19 and consequently exposed to the virus.”
This is a short list compared to other publications.
The authors then state that a major risk of a false positive result occurs when the individual is cohorted (hospitalized) with other patients suffering from COVID-19 and is consequently exposed to the virus, and the authors provide a case study.
The costs externalized to medicine that we experienced during the lockdown are proof that when we get it wrong at the population level, disaster awaits.
We certainly cannot mandate routine screening with PCR. It’s a leaky test - and variants have already escaped because mutations in the primer sites cause the tests to fail at even higher rates.
Take out the misuse of PCR (“PCR+ = COVID”), and this thing is over. We must show the truth via sequencing clinical samples. Our proposal is peer-reviewed and IRB approved; we need to sequence samples from 200 symptomatic patients who test positive via PCR and 200 symptomatic patients who test negative with PCR. We have clinical selected and the fall “flu” season is upon us.
NIH won’t fund this study. CDC won’t conduct it (in fact, they conflate their analyses intentionally to prevent awareness of these issues).
OSHA's ETS is internally inconsistent on the reliability of testing for COVID-19.
To justify why those immune from prior infection should not be exempt from their rule, OSHA writes (Section 1.B.3)
"Given scientific uncertainty and limitations in testing for infection and immunity, OSHA is concerned that it would be infeasible for employers to operationalize a standard that would permit or require an exception from vaccination or testing and face covering based on prior infection with COVID-19."
In citing the limitations in testing for infection, OSHA should recognize that this uncertainty applies equally to the vaccinated, the unvaccinated, and the previously immune. This means the assessment of the efficacy of the vaccines in the clinical trials itself should be scrutinized closely.
More importantly, OSHA should recognize that they cannot come to a determination of grave danger if the same testing methods used to determine the numbers of cases and deaths due to COVID-19, and to the estimates of the efficacy of the vaccines themselves, are unreliable, as OSHA has stated, and as published estimates demonstrating false positive rates have shown.
Pulling out the “PCR+ = COVID19” distortion means the clinical trial efficacies all have to be re-determined.
Pulling out the “PCR+ = COVID19” distortion means there is no trust in the OSHA ruling that mandates workplace screening.
Pulling out the “PCR+ = COVID19” distortion means that the official numbers of COVID-19 cases, breakthrough infections, and deaths all must be re-assessed.
That’s why this is so incredibly important.
We need to raise a ton of money fast to get this going. We are about 5% funded. See #NAATEC on social media and the link at the NAATEC Consortium page at the IPAK Website (click on the IPAK logo below). If you’ve already donated, please share this article everywhere.
The NAATEC Consortium Members are counting on you.
