


Scott Gottlieb, the Walking Embodiment of Conflicts of Interest and Regulatory Capture, Reveals that He Does Not Understand the State of Vaccine Science
Attacking Robert F. Kennedy, Jr. on CNBC in a world in which experts have pored over and analyzed the state of vaccine science in great detail for over ten years was a huge mistake.


In a recent CNBC segment, Dr. Scott Gottlieb, former FDA Commissioner and current Pfizer board member, issued dire warnings about “vaccine skepticism”, specifically targeting Robert F. Kennedy Jr. In the segment, Dr. Gottlieb portrayed himself as a champion of public health, but his statements were riddled with factual inaccuracies, oversights of critical scientific evidence, and an alarming disregard for emerging complexities in vaccine science.
This critique, building upon and reiterating some points brought up by superlawyer Aaron Siri on X , addresses Dr. Gottlieb’s commentary, corrects his claims, and highlights evidence from experts that he conspicuously failed to acknowledge.
Correcting the Record on Dr. Gottlieb’s Claims
1. The MMR Vaccine and Thimerosal: A Nonexistent Reformulation
Dr. Gottlieb stated that in the early 2000s, the FDA reformulated the Measles, Mumps, and Rubella (MMR) vaccine to remove preservatives like thimerosal. This claim is demonstrably false. The MMR vaccine has never contained thimerosal or any other preservatives.
Archived Evidence: The CDC explicitly states that "Measles, mumps, and rubella (MMR) vaccines do not and never did contain thimerosal.” (Wayback Machine Link).
Dr. Gottlieb’s inability to distinguish between vaccines containing thimerosal and those that do not is concerning for someone claiming expertise in public health.
2. MMR Vaccination Schedule: Ignorance of Routine Guidelines
Dr. Gottlieb claimed children cannot receive the MMR vaccine until age two, a blatant misrepresentation of the CDC’s immunization schedule. The first dose of MMR is routinely given at 12 months of age, with earlier administration recommended during outbreaks.
Archived Source: CDC’s immunization schedule confirms this fact (Wayback Machine Link).
3. Misleading Public on Pertussis Vaccine Transmission
Dr. Gottlieb failed to address the scientific consensus that acellular pertussis vaccines do not prevent transmission. Instead, they merely reduce symptoms in vaccinated individuals, potentially increasing the risk of asymptomatic spread.
Evidence from the FDA: Vaccinated individuals can still carry and transmit Bordetella pertussis. (See James Cherry’ paper especially and PubMed Link, h/t, Aaron Siri).
Analysis from Popular Rationalism: Vaccinated adults, particularly healthcare workers, may unknowingly spread pertussis, creating risks for infants and vulnerable populations. Those mostly include healthcare workers.
The implication that vaccination alone can protect against pertussis transmission misleads the public and policymakers alike.
4. Waning Immunity and Booster Overreach
Dr. Gottlieb’s blanket support for booster vaccinations ignores the reality of waning immunity. For instance:
Pertussis: The Tdap booster’s efficacy declines from 73% in the first year to 34% within 2-4 years (KQED Report).
SARS-CoV-2: Vaccine-induced immunity wanes within months, necessitating regular updates and raising questions about sustainable public health strategies.
Such omissions betray a lack of transparency and forthrightness about the limitations of vaccine efficacy.
5. Ignoring Non-Specific Effects and Population-Level Adverse Events
Dr. Gottlieb did not address emerging evidence on the non-specific effects (NSEs) of vaccines, which can include both benefits and harms at the population level.
Research from Guinea-Bissau: Two key studies, Aaby et al. (2018) and Mogensen et al. (2017), have raised important questions about the non-specific effects of the Diphtheria-Tetanus-Pertussis (DTP) vaccine on child mortality.
Aaby et al. (2018) found that children who received the DTP vaccine in Guinea-Bissau experienced a 1.89-fold increase in all-cause mortality compared to unvaccinated children, with the effect being particularly pronounced among girls. The study suggested that the increase in mortality was not due to the target diseases (diphtheria, tetanus, or pertussis) but potentially linked to other causes, such as pneumonia or sepsis.
Similarly, Mogensen et al. (2017) examined the introduction of the DTP and oral polio vaccines among infants aged 3–5 months in the same region. The study reported higher mortality rates among vaccinated children compared to their unvaccinated peers, again with a more pronounced effect in girls. These findings aligned with the earlier observations, strengthening the case for further investigation into sex-differential responses to the DTP vaccine.
Together, these studies highlight a potential pattern of increased all-cause mortality associated with DTP vaccination, raising critical questions about vaccine schedules, co-administration practices, and the underlying biological mechanisms driving these effects.(BMJ, 2016).
The failure to consider these complexities reflects Gottlieb’s narrow and outdated understanding of vaccine science.
Conflicts of Interest and Misrepresentation
Dr. Gottlieb deflected concerns about his role on Pfizer’s board by claiming Pfizer does not manufacture pediatric vaccines. This is patently false.
Pfizer’s Prevnar Vaccine: A leading product in the pediatric market, Prevnar is administered to infants at 2, 4, 6, and 12 months and is a top revenue generator for Pfizer. (Pfizer Financial Report). (h/t, Aaron Siri)
Dr. Gottlieb’s denial raises questions about transparency and accountability.
A Pattern of Oversimplification and Misleading Claims
Dr. Gottlieb’s commentary on CNBC follows a troubling pattern of oversimplifying vaccine science:
Polio Vaccination: Gottlieb ignored the fact that the inactivated polio vaccine (IPV) does not prevent viral transmission, undermining herd immunity (Plos).
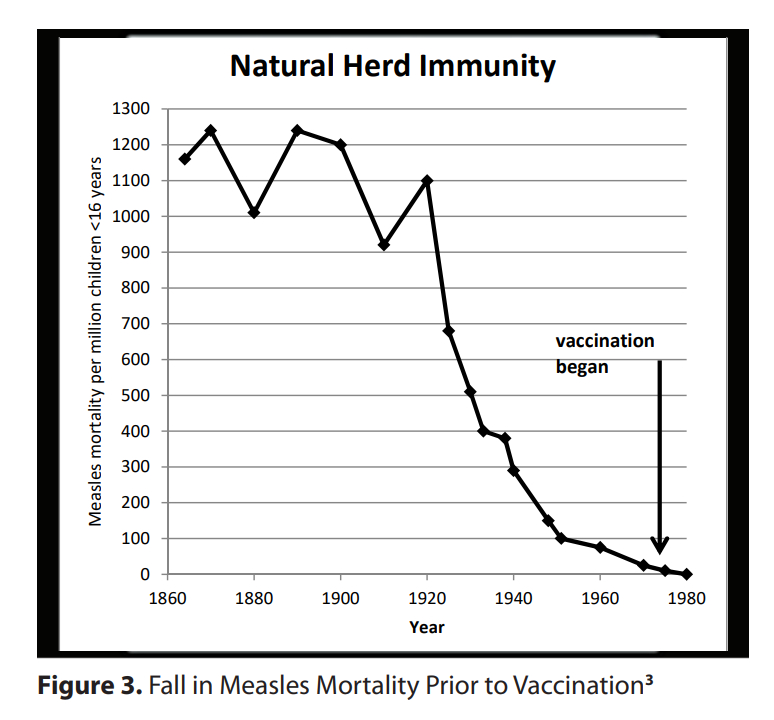
Measles Mortality: Gottlieb inflated claims about pre-vaccine measles deaths fail to account for a 98% decline in mortality before the vaccine’s introduction, attributable to improved public health infrastructure, according to national vital statistics (McKeown T. The Modern Rise of Population. Academic Press; 1976), which reported that vaccines are given too much credit for the decline.
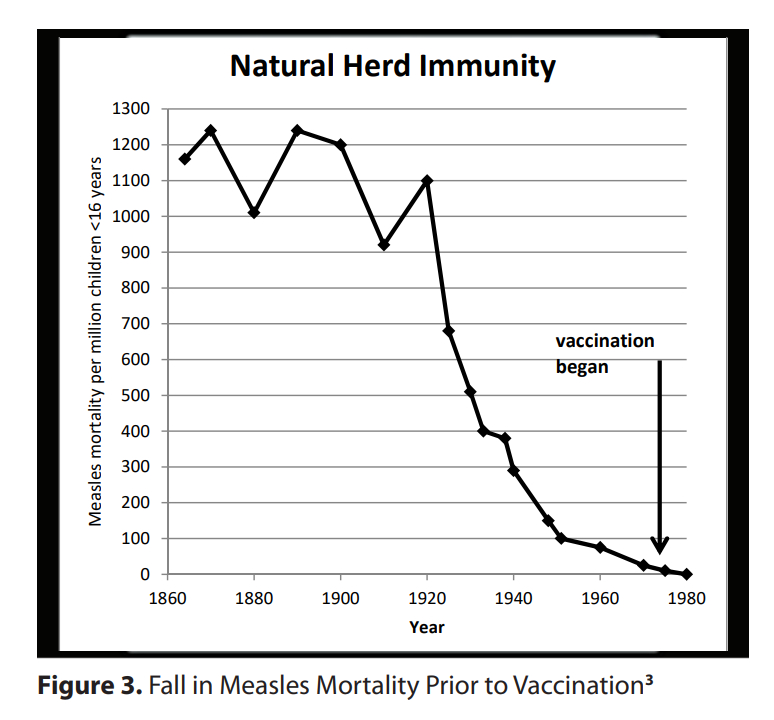
This figure is from Dr. Wakefield’s in-depth, thoughtful analysis.
These positions held by Gottlieb \suggest an agenda-driven narrative rather than a commitment to evidence-based discourse.
Conclusion: A Call for Evidence-Based Dialogue
Dr. Scott Gottlieb’s CNBC appearance exemplifies the dangers of conflating corporate interests with public health advocacy. His misleading claims and conflicts of interest undermine public trust in vaccines and the institutions that are supposed to safeguard them.
We urgently need transparent, evidence-based discussions about vaccine efficacy, limitations, and broader implications. Highly visible public personalities like Dr. Gottlieb must be held accountable for their public statements to ensure the integrity of public health policy. Only through rigorous analysis and honest dialogue can we address the challenges facing vaccination programs and restore confidence in their role as critical tools for disease prevention.
Outstanding article! Scott Gottlieb surely will become a relic in American Public Health discourse!
Criminal in Action (CIA)