


Now That Children and Young People (CYP) Are Being Vaccinated, JAMA Study Reports Death From COVID-19 Has Become a Leading Cause of Death: Death Rate Greater than Before Vaccination in Children
JAMA Study is agnostic to vaccine-induced immunosuppression, ADE, immunotolerance, and other problems we all know too well.

NB: Every lost child is a catastrophe. Nevertheless, we must consider the consequences of this JAMA report in terms relative to “before vaccination”, which the authors did not.
Quick Take-Home: The JAMA Report does not provide sufficient information about the study population to attribute the deaths to COVID-19 alone. In general, pediatric death rates are likely inflated due to PCR false positives. Why the study did not make appropriate comparisons to CDC Wonder data in a period before the COVID-19 vaccination is not clear. Why the study did not study the incidence of deaths per confirmed infection is also a mystery.
May 12, 2021: The Centers for Disease Control and Prevention (CDC) approved the use of the Pfizer-BioNTech COVID-19 vaccine in persons aged 12-15 years.
August, 2022: FDA approved a BLA for the Pfizer-BioNTech COVID-19 vaccines in persons >15 years of age, and the same vaccine was authorized under EA for children and adolescents aged 5-15 years.
November 2, 2021: CDC recommended Pfizer’s COVID-19 vaccine for children, ages 5-11.
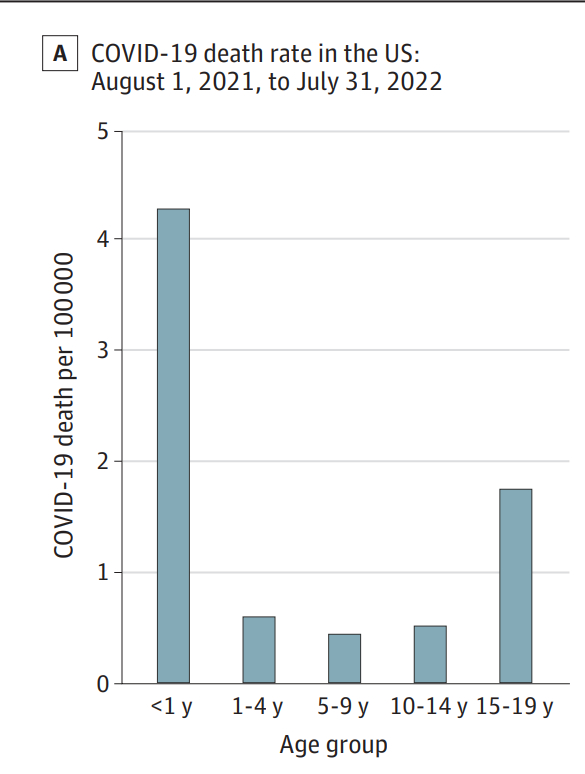
According to recent a study in JAMA, in the 1-year period from August 1, 2021, to July 31, 2022, COVID-19 became the 8th leading cause of death in children and young people (aged 1-19 years) in the US. The study was a national population-level cross-sectional epidemiological analysis for the years 2019 to 2022. The authors of the report used data from the US Centers for Disease Control and Prevention’s “Wide-Ranging Online Data for Epidemiologic Research” (WONDER) database on the underlying cause of death in the US.
Oddly, rather than comparing post-vaccine era deaths due to COVID-19 to pre-vaccine era deaths in this age group, the report ignores the clear indication that COVID-19 vaccinations may be making the SARS-Cov-2 virus more deadly for the young.
Instead, the authors of the JAMA report decided to compare deaths in CYP from COVID-19 with deaths from other vaccine-targeted diseases historically. They wrote:
“COVID-19 caused substantially more deaths (821 deaths in our study period in CYP) than major vaccine-preventable diseases did before vaccines became available: hepatitis A (3 reported deaths in children per year in the US), rotavirus (20-60 reported deaths in children per year in the US), rubella (17 reported deaths in children per year in the US), varicella (50 reported deaths in children per year in the US),15 and measles (495 total reported deaths per year,16 the vast majority in children17).”
A reader wrote to me this morning about this editorial from Paul Offit about a different study. Offit cited similar rates of deaths of these vaccine-targeted childhood illnesses, and the reader wrote:
“I do not remember seeing his editorial from last week discussed anywhere. He's pushing covid vax for kids based on 66 deaths in a one-year period (no explanation of comorbidities -- or vitamin d deficiency) and saying myocarditis in children aged 5-12 is 1 in 500,000, and generally short-lived and self-resolving. No word on other adverse events.
And he ADMITS (but presents it not ad admission but as a proud claim):
(Offit:) “Every year, prior to the availability of a vaccine, 3 children died of hepatitis A virus,10 8 children died of meningococcus,9 16 children died of varicella,11 17 people of all ages died of rubella,12 and 20 children died of rotavirus.13“
She continued:
That's out of what, 50 MILLION children age 0-13? Were those the children with cancer, or malnutrition, or no access to basic medical care? For those numbers, (why do ) we need THOSE vaccines?????? And that prompts the need for the 66? How many might have been fine if treated with vitamin D?”
Why Did They Compare COVID-19 Deaths from a Vaccination Period to Non-COVID-19 Vaccine-Targeted Illnesses Pre-Vaccination Period?
This is an odd tact to the analysis because their data on COVID-19 CYP deaths were collected over the timeframe when COVID-19 vaccines were approved for children. The study did not report how many of the 821 children were exposed to any dose of COVID-19 jabs.
They also reported:
“(Over this time period), (a)mong children and young people aged 0 to 19 years in the US, COVID-19 ranked eighth among all causes of death, fifth in disease-related causes of death (excluding unintentional injuries, assault, and suicide), and first in deaths caused by infectious or respiratory diseases. COVID-19 deaths constituted 2% of all causes of death in this age group.”
A 2021 report from England conducted before vaccination in this age group, only 2 out of every million people in the CYP age group from March 2020 to Feb 2021.
See: “Deaths from COVID ‘incredibly rare’ among children: Studies find that overall risk of death or severe disease from COVID-19 is very low in kids.” (Nature).
According to STATISTA, about 82,130,000 people aged 0 to 19 years are in the US.
With 821 deaths attributed to COVID-19, the COVID-19-attributed death rate over the year period in the JAMA study is about 10 per million.
This suggests that the COVID-19 vaccination program has increased the death rate 5-fold in children and young people compared to the UK data.
Note that the majority of deaths attributed to COVID-19 in their data are in infants under 1 year of age, and also note that the JAMA Report does not adjust for the now firmly established fact of a non-zero, likely very high false positive rate of the PCR test for the diagnosis of COVID-19.
CDC did not start recommending COVID-19 vaccines for infants and toddlers until June 18, 2022 (ages 6 mos to 4 years), so we need age group-specific comparisons. Roughly about 36% of the deaths attributed to COVID-19 in the JAMA report are in the age range of 5 to 19 years old, so the rate increase in deaths in the vaccinated groups might be reasonably adjusted to 1.8 times for 5-19 year-olds compared to the period before COVID-19 vaccines instead of 5 times.
August 2021 was the Turning Point
Recall that in August, 2021: FDA approved a BLA for the Pfizer-BioNTech COVID-19 vaccines in persons >15 years of age, and the same vaccine was authorized under EA for children and adolescents aged 5-15 years.
The JAMA report shows an increase in the rates of death from COVID-19 starting in August, 2021.

Of course there is a seasonality in the number of cases, so this chart ideally would be deaths per confirmed case, not merely the number deaths.
According to the American Academy of Pediatrics, the rates of vaccine uptake in children have varied with State, ranging from 17% to 81%. The JAMA report should have reported the vaccination status of the children who died, and they should have calculated the rates of death in vaccinated vs. unvaccinated children per age group. Importantly, they also should have considered whether the children had received thimerosal-containing influenza vaccines, given that thimerosal disrupts the human immune system protein ERAP1.
However, the age group-specific numbers are likely too low for reliable estimates, especially after correcting for false-positive rates of PCR. The UK pre-vaccine CYP death rate data were also not adjusted for PCR false positives, so the relative rates might be comparable.
However, we cannot assume the false positive rate is constant over time because it is widely known and accepted among virologists like Andrew Rambaut that the virus evolves away from the PCR test as it is implemented. This means we can reasonably expect a higher rate of COVID-19 misattribution in the latter period.
Popular Rationalists will understand that this also therefore means the higher rate in the latter period could be, at least in part, an artifact of increased testing rates and increased false positives in those tests.
Conclusion: The JAMA Report does not provide sufficient information about the study population to attribute the deaths to COVID-19 alone. In general, pediatric death rates are likely inflated due to PCR false positives. Why the study did not make appropriate comparisons to CDC Wonder data in a period before the COVID-19 vaccination is not clear. Why the study did not study the incidence of deaths per confirmed infection is also a mystery.
The JAMA Report:
What mystery?
The purpose of the study obviously was to appear to be seeking objective truth on covid deaths in children, while actually trying to avoid drawing attention to any concerns about efficacy or safety.
To quote the old fasco-Marxist leftist meme, "It's the SHOTS, stupid." As in ADE/PIE immune suppression.
Funny thing. Until the immune suppression from the shot kicked in, kids death was basically ZERO.
Dr. Jay Bhattacharya, PhD, MD, Stanford Medical School said Oct. 2020 in Imprimus that kids under 21 have ***two to three times the deaths from regular, seasonal flu than they due Covid."
Dr. Makary at Johns Hopkins University Bloomberg School of Medicine with other scientists teamed up with the non-profit FAIR Health group to look at the insurance data of 48,000 children diagnosed with Covid between April 2020 and Aug. 2020. Not ONE of the children who died were free of pre-existing medical conditions such as cancer https://www.naturalhealth365.com/zero-covid-death-among-children-3920.html (see also here: https://www.theburningplatform.com/2021/10/06/covid-jabs-could-potentially-kill-thousands-of-kids-former-hhs-epidemiologist/ ). And this is true in Germany, too, where a massive study late fall showed ZERO – there’s that word again – deaths from Covid among healthy German kids, as reported by Alex Berenson here, Dec. 2, 2021 https://alexberenson.substack.com/p/huge-new-study-shows-zero-covid-deaths , or here at LifeSite News. https://www.lifesitenews.com/news/study-debunks-need-for-kid-covid-shots-not-one-healthy-german-child-under-18-died-from-virus/
Or see a the details in a late 2021 German study https://www.medrxiv.org/content/10.1101/2021.11.30.21267048v1.full.pdf (collating evidence from three sources 1) a national seroprevalence study (the SARSCoV-2 KIDS study), 2) the German statutory notification system and 3) a nationwide registry on children and adolescents hospitalized with either SARS-CoV-2 or Pediatric Inflammatory Multisystem Syndrome (PIMS-TS)) reported that there were zero (0) deaths in children 5 to 18 years old across the period of study.
Ditto in Sweden - Swedish data by Ludvigsson https://pubmed.ncbi.nlm.nih.gov/33406327/ reported on the 1,951,905 children in Sweden (as of December 31, 2020) who were 1 to 16 years of age who attended school with largely no lockdowns or masks. They found zero (0) deaths. “Despite Sweden’s having kept schools and preschools open, we found a low incidence of severe Covid-19 among schoolchildren and children of preschool age during the SARS-CoV-2 pandemic.” If you include kids with serious morbidities, there were six deaths. In Germany, out of a total population of 80 million, around 10 million school age kids. Even serious illness was extremely rare, 1 in 50,000. See Dr. Paul Elias Alexander’s SWEDEN AND GERMANY: NO DEATHS IN CHILDREN DUE TO COVID for more reading here https://brownstone.org/articles/sweden-and-germany-no-deaths-in-children-due-to-covid/ , or this article which notes that German scientists found that no healthy child 5-17 years of age died of COVID in Germany https://www.clarkcountytoday.com/news/autopsy-study-ties-deaths-to-covid-vaccine/