


Looking Back at Delta, This Research Team Engaged, Forewarned, and Were Ignored
The Epidemiologic data showed that Delta was less deadly compared to prior variants, but prior immunity might be the explanation. This team detected part of the story but were careful.

I will encourage my readers to see the type of “holding back” that has to be conducted to get published in so-called “main stream” scientific journals. From Dec 2021 until the present day, a team of researchers from California published three articles and one letter in which they they have tried to warn that the vaccinated, especially the older vaccinated population, were at risk of dying in spite of the vaccination.
A Dr. Venkat Emani sent me this summary along with copies of four publications. Here are the four publication:
Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant
Here, they warn that evolution is making the vaccine against the Wuhan-type virus obsolete. Knowing this, read their communication and how careful they have to word that important message.
Now read
“However, the Public Health England briefings also show a growing problem of COVID-19 breakthrough cases in the ≥ 50 years age group, with fully vaccinated share of breakthrough cases increased from 37.0% in briefing 17% to 75.3% of breakthrough cases among fully vaccinated as of September 12, 2021 reporting period in briefing... This was associated with 67.0% of subgroup deaths in the fully vaccinated in ≥ 50 years age group. This was probably due to waning of vaccine efficacy and fully vaccinated high-risk population not taking preventive measures to avoid exposure which need further investigation.”
Here, in this paper, they reported pre-existing conditions presenting as risk factors for death from COVID-19 infection:
What I appreciate about this is that they did not merely consider these conditions (like diabetes, and asthma, etc) as “co-morbidities” but rather “risk factors”, which leaves open the causal pathway because risk factors are not necessarily confounder that should be adjusted for in, say, studies of vaccine safety. Their word choice is subtle and careful, but makes all the difference.
In fact, their cautious approach (if followed by others) would leave it open that perhaps studies of vaccine safety and of COVID-19 health outcomes might be conducted on people in these risk factors as subgroup analysis.
In the next analysis they sent to me, they cited a study that allegedly showed that COVID-19 vaccines reduced mortality in nursing homes in the UK. A quick look at that study’s methodology shows they used adjusted Hazard Ratios to calculate vaccine efficacy… here’s the language:
“The baseline hazard was defined over calendar time. We adjusted for sex (as a binary variable), age (as a cubic spline term), evidence of previous SARS-CoV-2 infection (as a binary variable), long-term care facility bed capacity (as a linear term), and monthly SARS-CoV-2 incidence for the local authority in which the long-term care facility was located (as a linear term).”
(Bear with the statsci-chitter-chatter here, hang on for the duration of this article, be glad I’m not mentioning eignvectors): I question the appropriateness of adjusting for so many covariates rather than doing subgroup analysis (e.g., gender, clearly). And adjusting for age really confounds the results with a risk factor (to my prior point). Some causal link between long-term care facility bed capacity and vaccine efficacy should have been justified to treat it as a covariate worth adjusting, and local SARS-CoV-2 incidence should related to internal infection rate, sure, but linear? And why not block instead adjust?
And look at the cited study’s results:
“In Cox regression analyses, we found no significant reduction in hazards of PCR-positive infection until 28–34 days after vaccination (adjusted HR 0·44, 95% CI 0·24–0·81; table 3). At 35–48 days, the adjusted HR was similar to that at 28–34 days at 0·38 (95% CI 0·19–0·77), equating to a vaccine effectiveness of 62% (95% CI 23–81). At 49 or more days, the estimates were much less precise and no longer significantly different compared with the unvaccinated group (adjusted HR 0·49, 95% CI 0·20–1·17). In this adjusted model, previous infection was strongly associated with a reduced hazard of subsequent infection (adjusted HR 0·19, 0·12–0·30).”
But far more importantly, what happened up to 28-34 days (and why a range??). I plotted the data from the cited study:
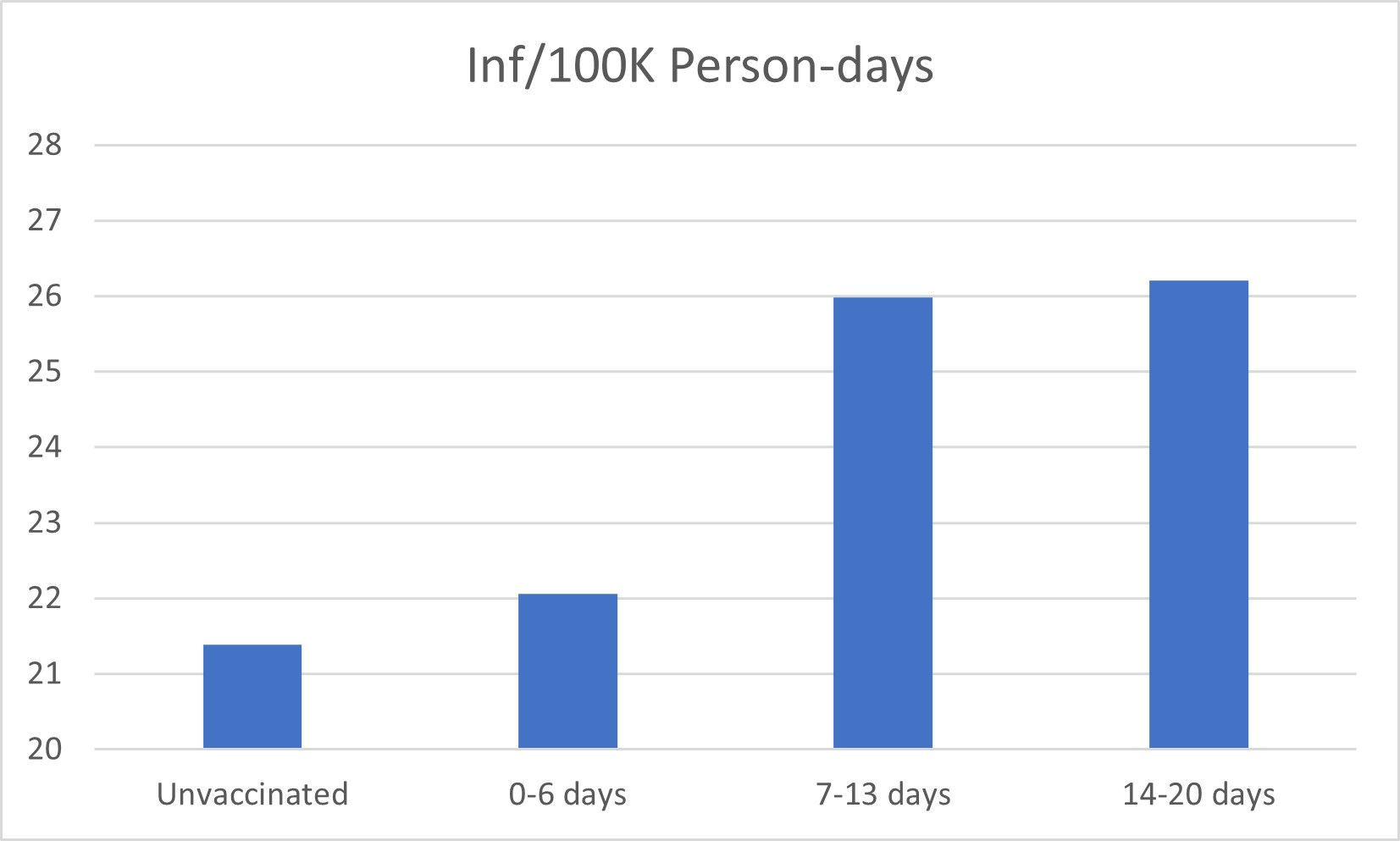
The rest of the data are available online at the study publication site.
Note that Dr. Emani’s research team did not emphasize this part of the result (there is clearly a significant trend!), I presume because it would condemn the vaccine for ADE - leading to infections in those vaccinated and unvaccinated due to higher spread directly following the vaccination. To me this is being too cautious. This pattern was noted in other nursing homes data, and leads to the question: why would anyone put those most at risk at higher risk of infection? Would that not put others at higher risk of death as well, especially if the vaccine impairs immunity for a time, as we now suspect it does?
To their credit, Dr. Emani cited “prior COVID-19 infection” as an equally likely variable that could explain the drop in infection rate following their citation of this flawed study they dare not critique.
Even in their email summary to me, the team was cautious:
“Our publications on UK Delta variant: Summary of the four publications
The Delta variant surge is associated with significantly lower mortality and hospitalizations than the Alpha variant. As the Delta variant surge progressed, ≥ 50 years old had a significant increased percentage of cases, hospitalizations and a significant increased COVID-19 deaths occurred among ≥ 70 years old age group.
The majority of deaths (93.5%–94.8%) among those older than 60 years of age during the Delta variant surge were associated with preexisting conditions, with a slight but statistically significant increased proportion of deaths in those without preexisting conditions (7.7% vs 4.1%) during the Delta variant surge than the prior comparision (sic) period before the Delta variant surge.
Over 50 yrs population has 57.4% of cases in fully vaccinated with 2 doses, 51.5% of hospitalizations and 53.0% of deaths occurred in fully vaccinated adults by July 23, 2021 as noted in our published letter in NEJM as correspondence.
History of breakthrough cases during Delta variant surge in UK: the Public Health England briefings show a growing problem of COVID-19 breakthrough cases in the ≥50 years age group, with fully vaccinated share of breakthrough cases increased from 37.0% in briefing 17 to 75.3% of breakthrough cases among fully vaccinated as of September 12, 2021 reporting period in briefing 23. This was associated with 67.0% of subgroup deaths in the fully vaccinated in ≥50 years age groups.
A significantly lower number of COVID-19 deaths occurred in care homes during the Delta variant surge in England and Wales; the number of care home deaths caused by COVID-19 was significantly lower than the prior surges
Clinical relevance of the data
Over 50 yrs (particularly over 70 yrs) and or persons of any age with preexisting conditions should take universal precautions to avoid COVID infections.”
Here’s my take: The reality is that most people practicing medicine see what has happened, and to the extent they want to avoid undue persecution for stating the obvious, they publish what they can get away with to fly under the radar of the Taliban-like medical boards who answer to top-down imposed “standards of care”. In reality, the standard-of-care model should come from the bottom-up - always - and be based on real-world data leading to clinical trials in search of consensus of results.
In the fourth publication, the team reported, among other findings, higher risk of breakthrough infection in the elderly following the third booster based on the analysis of all data from Israel (See: SARS-CoV2 Breakthrough Infections in Elderly Third Booster and Vaccinated Population Considered Vaccine Immune During Omicron (B.1.1.529)Variant Surge in Israel). They conclude that the elderly must be protected (by other means, the reader is left to presume).
To my knowledge, this particular team has not published on the critical data compiled and available at http://c19study.com or https://ivmmeta.com/. Their primary concern is the increased risk of death in the elderly, so it would interesting to see their take on the significance of the actions of Fauci and others to bury the data on the importance of early treatment, which many increasingly see as the primary cause of death due to COVID-19.
The point for writing this up is to give the team credit for coming as far as they could warning the world against the perils of the vaccine. It’s time now, however, for all research scientists and physicians who know what is going on to step out loudly and boldly and to be brave enough to state what they mean clearly an on-point. We cannot win back our rights to objectivity in science and freedom to educate each other about reality if we have to hedge on reality. I’ve invited Dr. Emani to comment on this article; I hope he does, and I hope this article is sent to many medical professionals who have yet to learn (or who won’t admit they know) that there is something terribly, terribly wrong with the vaccination program, as Dr. Fantini predicted, and that public health overstepped into allopathic medicine, overruling medical approaches to reducing morbidity and mortality from SARS-CoV-2 infection in their campaign to make the vaccine the supreme measure of control, and denying the data that shows record levels of vaccine adverse events and deaths. They have failed. And they have done more harm than good by turfing effective means of treating the illness and substituting ten days of “getting as sick as you can” before coming for emergency care.
By the way, we’re teaching a course, “The Math of Vaccine Science” this summer at IPAK-EDU (starting in June). The course will be led by a tenured Epidemiologist. Annual subscribers to Popular Rationalism can receive 20% of any course at IPAK-EDU! In this summer course, we’ll be examining simple and more complex issues in vaccine studies and teaching the public all of the details of the common analyses used in vaccine studies. Be sure to sign up for that class if you want to be able to jump into any vaccine study and by able to know the expected effects of decisions made about the methods of analysis on the outcome of the study.

You are really too kind in your language. Research funding in the control of govt. agencies makes all researchers whores, to greater or lesser extents; that's just built into the system. I think Eisenhower warned us about that in addition to the Military/Industrial Complex.
But this has been true since the beginning of formal educational institutions. First they were controlled by priesthoods under the auspices of monarchs. Not much difference now.
Look the ONLY thing the world needed to do was NOT aggregate old people who had the flu together. PERIOD