


Intentional Abuse of Health Outcomes in Studies and Recommendations of Vaccines During Pregnancy
A Critical Examination of Scientific Integrity, Data Suppression, and Ethical Failures in Vaccine Safety Research

“They mysteriously stopped the trial after 349 women enrolled in the study … the results of those 349 women have never been made public” - Dr. Marty Makary
The Helsinki Declaration, first adopted in 1964 by the World Medical Association, was designed to protect human subjects in medical research. It mandates that scientific progress must never take precedence over individuals' rights, well-being, and autonomy. In the context of vaccine recommendations for pregnant women, however, these ethical principles were systematically ignored.
The Helsinki Declaration vs. Reality
Medical research is governed by ethical principles designed to prioritize patient safety, well-being, and autonomy above all else. The Helsinki Declaration, which has guided human research ethics since 1964, provides a clear framework for responsible scientific conduct. However, the response to the COVID-19 pandemic—and the vaccine recommendations for pregnant women in particular—flagrantly violated these ethical standards.
First Principle: "The health of my patient will be my first consideration."
Physicians are ethically bound to assess risk and benefit for each individual patient.
However, COVID-19 vaccine recommendations for pregnancy were issued without individualized risk assessments. Instead, universal mandates and coercive messaging were implemented, forcing compliance without adequate consideration of potential risks.
"It’s safe to have the vaccine during any stage of pregnancy." – UKHSA, CDC
This unwavering certainty contradicted the actual regulatory package inserts, which openly acknowledged a lack of safety data for pregnancy:
“No data are available yet regarding use during pregnancy.” (EMA, MHRA)
“The available data on COMIRNATY administered to pregnant women are insufficient to inform vaccine-associated risks in pregnancy.” (US FDA)
“The safety and efficacy of COMIRNATY in pregnant women have not yet been established.” (Health Canada)
Despite these admissions, governments and health agencies aggressively promoted the vaccine, claiming it was proven safe and necessary. This violated the foundational principle that physicians must prioritize the health of individual patients over political or economic agendas.
Clause 8: "The primary purpose of medical research is to generate new knowledge, but this goal can never take precedence over the rights and interests of individual research subjects."
Informed consent is the bedrock of ethical medicine. However, during the COVID-19 vaccine rollout, pregnant women were actively discouraged from questioning the available data. Those who hesitated faced social pressure, workplace mandates, and even denial of medical care.
Additionally, research on COVID-19 vaccines in pregnancy was not designed to generate meaningful knowledge about risks. The Pfizer pregnancy trial (C4591015) was supposed to be the gold standard for safety assessment—but it was drastically reduced in size and terminated early, ensuring that no meaningful conclusions could be drawn.
This represents a clear violation of Clause 8, as regulatory agencies and public health authorities prioritized global vaccine coverage over the protection of individual patients' rights.
Clause 9: "Physicians involved in research must protect life, health, dignity, and self-determination of participants."
One of the most egregious ethical violations was coercing pregnant women to receive a vaccine that had not been adequately tested in their demographic.
Doctors who advised caution faced professional retaliation.
Pregnant women who refused vaccination were stigmatized and, in some cases, denied services or employment.
Informed consent was reduced to a formality, with misleading messaging erasing uncertainty about vaccine safety.
These actions directly contradicted the Helsinki Declaration’s demand that medical professionals uphold dignity, integrity, and self-determination in medical decisions.
Public health agencies, regulatory bodies, and pharmaceutical companies made bold, unequivocal claims about the safety of COVID-19 vaccines during pregnancy before adequate safety data existed. The pandemic saw an unprecedented global push to vaccinate pregnant women under the banner of “trusting the science”, even when the science itself was incomplete, selectively reported, or outright suppressed.
One of the defining features of regulatory capture is the revolving door between government agencies and pharmaceutical corporations. Many top decision-makers within the CDC, FDA, EMA, and WHO have previously worked for or later moved into lucrative positions within pharmaceutical companies. This raises serious ethical concerns about conflicts of interest.
Scott Gottlieb, former FDA Commissioner, became a Pfizer board member after leaving the agency.
Janet Woodcock, an FDA official, played a role in the approval of numerous controversial drugs, including opioids, before becoming Acting FDA Commissioner.
Former CDC officials routinely take high-paying positions in the pharmaceutical industry, effectively ensuring that regulators remain loyal to the corporations they once regulated. An example of this is Julie Gerberding, who was the director of the CDC from 2002 to 2009 and who accepted an extremely lucrative position at Merck in leadership on vaccines.
With this deep financial entanglement between regulators and industry, it is no surprise that vaccine safety concerns in pregnancy were dismissed rather than investigated.
The 2009 H1N1 influenza vaccine program serves as a critical historical precedent for these failures. Emerging data from VAERS and independent analysts suggested a significant increase in spontaneous abortions and stillbirths following the 2009 H1N1 vaccination campaign. Yet, these findings were dismissed, omitted from official presentations, and ignored by public health authorities. The COVID-19 vaccine rollout replicated these failures on a global scale with even greater manipulation of data, premature trial terminations, and regulatory mismanagement.
Through data suppression, the selective reporting of adverse events, and manipulated study designs, regulatory agencies and pharmaceutical companies created a misleading narrative that erased the very real risks posed by these vaccines to fetal development and maternal health. Meanwhile, dissenting scientists and physicians who raised concerns about the inadequate safety data were censored, discredited, or professionally threatened.
This article will critically examine how vaccine safety research in pregnancy has been systematically compromised, exposing:
The suppression of adverse event data
The selective use of VAERS reports to manipulate risk perception
The flaws in key vaccine trials, including the COVID-19 pregnancy study (C4591015)
How regulatory agencies promoted false safety claims
Without transparency, independent oversight, and ethical research practices, public trust in vaccine safety will continue to erode—not due to misinformation, but due to the systematic deception carried out by the very institutions tasked with protecting public health.
The Shimabukuro Incident: Omitted Data and Suppressed Risks
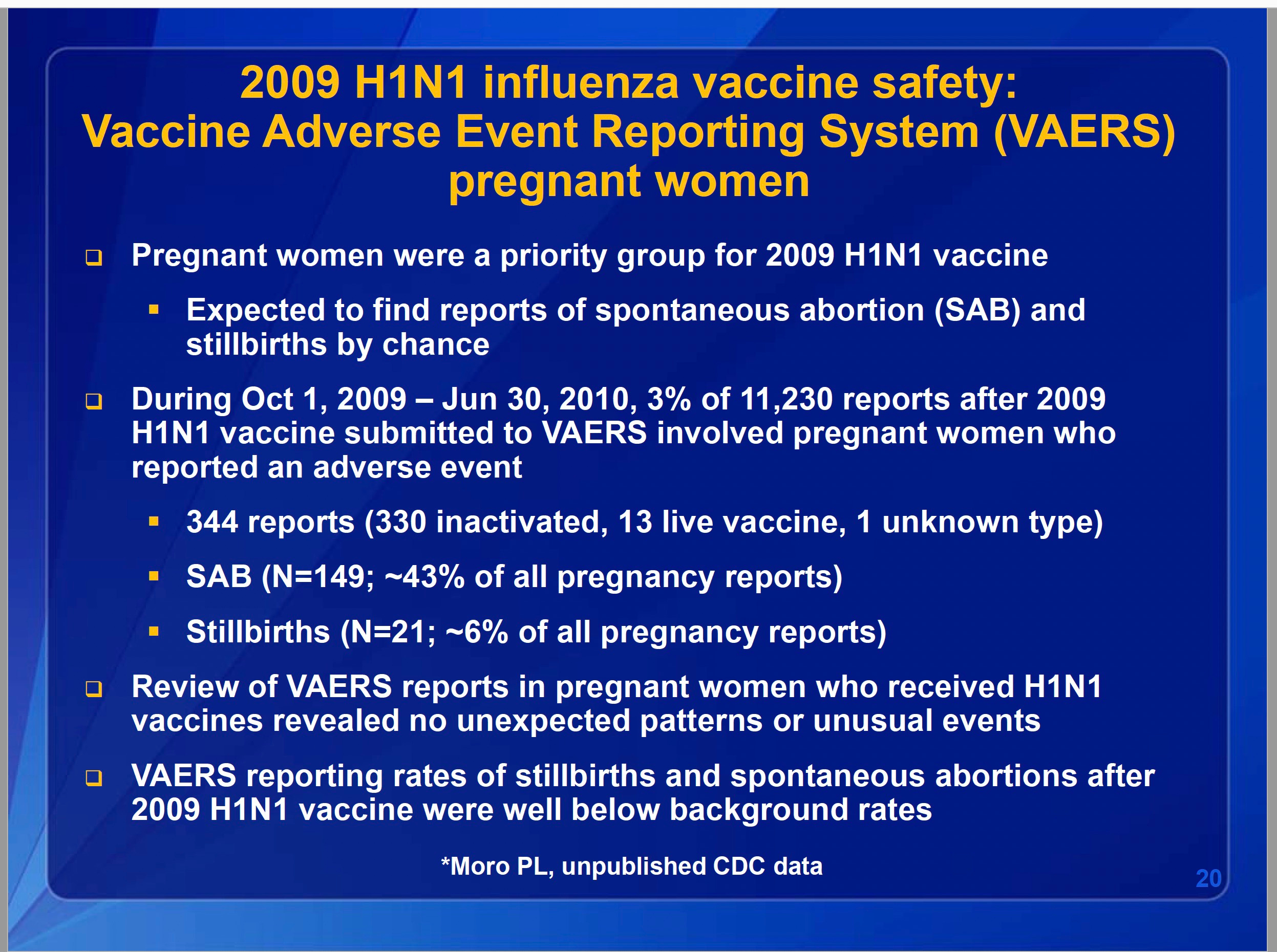
Dr. Thomas Shimabukuro, a senior scientist at the CDC’s Immunization Safety Office, presented vaccine safety data to the Advisory Committee on Immunization Practices (ACIP) in 2010. His official report included a review of VAERS (Vaccine Adverse Event Reporting System) data on pregnancy-related adverse events following the 2009 H1N1 vaccine.
Key VAERS Findings on Pregnancy Outcomes:
344 pregnancy-related reports were submitted to VAERS.
149 cases (~43%) involved spontaneous abortion (SAB).
21 cases (~6%) were stillbirths.
These numbers should have raised serious concerns about the potential risks of the vaccine in pregnancy. However, the most alarming aspect of Shimabukuro’s presentation was not what he showed—but what he deliberately left out.
“He purposely excluded it from his presentation. So much deception went on, which we caught in real time.” – Eileen Dannemann
When directly asked about pregnancy loss data, Shimabukuro produced a slide that had been omitted from his official presentation. This slide showed a significant spike in fetal death reports in the 2009/2010 flu season compared to prior years.
Had Dr. Tocco not directly asked about pregnancy outcomes, this data would have remained hidden.
The CDC continued to push the vaccine as safe despite these findings, failing to initiate any further studies to investigate the potential risks.
The Gary Goldman Analysis: A 4,250% Increase in Fetal Death Reports
In response to the alarming VAERS pregnancy loss data, Dr. Gary Goldman, a former independent CDC contractor, conducted his own statistical analysis of vaccine-related pregnancy loss.
Using VAERS data and an independent secondary source, Dr. Goldman calculated a 4,250% increase in spontaneous abortion reports following the 2009 H1N1 vaccine.
This analysis suggested a massive safety signal, yet the CDC never formally investigated it.
Instead of addressing these concerns, the CDC continued to claim that “no unexpected patterns or unusual events” were found in the pregnancy safety data.
This deliberate dismissal of concerning safety signals set a dangerous precedent—one that would later be repeated during the COVID-19 vaccine rollout. The 2009 H1N1 vaccine rollout stands as a precedent for the suppression of pregnancy-related adverse event data.
Eyewitnesses at the ACIP meeting—including Eileen Dannemann, Director of the National Coalition of Organized Women—reported that Shimabukuro omitted a crucial slide that showed a dramatic rise in fetal death reports. When pressed by Dr. Renee Tocco Hunter, he pulled out a separate slide, which had not been included in the public presentation. This slide confirmed a significant spike in fetal death reports in the 2009/2010 flu season compared to prior years.
Had Shimabukuro not been directly questioned, this data would have remained hidden from public scrutiny. The CDC dismissed the data and continued to recommend the vaccine, failing to initiate any meaningful follow-up studies.
The 4,250% increase in spontaneous abortion reports calculated by Dr. Gary Goldman, an independent analyst, was ignored. Despite the clear safety signal, the CDC denied any unexpected adverse trends.
Here is the missing slide never shown the full committee:
Instead of addressing the safety concerns, Shimabukuro dismissed the findings, ensuring that no structural changes to vaccine safety oversight were implemented. This failure laid the groundwork for similar negligence during the COVID-19 pandemic.
The Pfizer COVID-19 Pregnancy Trial (C4591015): A Case Study in Scientific Misconduct
During the COVID-19 pandemic, regulatory agencies once again pushed an experimental vaccine on pregnant women without proper safety data. The Pfizer-BioNTech BNT162b2 (Comirnaty) vaccine was aggressively promoted for pregnancy before the completion of any well-designed trials.
The Pfizer pregnancy trial (C4591015) was originally intended to enroll 4,000 participants but was abruptly downsized to just 348 maternal participants before being prematurely terminated. This drastically reduced sample size ensured that the trial was underpowered to detect rare but serious adverse outcomes.
Moreover, the study excluded first-trimester pregnancies, meaning that no data was collected on the most critical period for fetal development. This exclusion eliminated any possibility of detecting teratogenic effects, despite the fact that first-trimester exposure is the most relevant time frame for assessing congenital malformation risks.
Even within the small and flawed dataset, concerning trends emerged. Pregnant women who received the vaccine showed an elevated relative risk for congenital malformations (RR = 1.67), adverse events of special interest including developmental delays (RR = 2.5), and preeclampsia (RR = 2.02).
Yet, instead of expanding the trial to investigate these trends, Pfizer and regulators terminated the study early, ensuring that long-term safety data would not be collected. Despite these severe methodological limitations, regulatory agencies falsely presented the vaccine as "proven safe" for pregnant women.
The Playbook: Manipulating Data to Hide Risks
Throughout the COVID-19 pandemic, public health agencies and pharmaceutical companies utilized a range of statistical manipulations to obscure potential vaccine-related risks, particularly those affecting pregnant women. These tactics were not novel; rather, they followed a pattern first observed during the 2009 H1N1 vaccine campaign, where selective reporting, reclassification of data, and premature study terminations created a misleading perception of safety. The same techniques were once again deployed in the COVID-19 era to construct a narrative that erased concerns about vaccine-associated pregnancy complications.
One of the most widely used methods of data manipulation was the reclassification of vaccinated individuals as “unvaccinated” for a specific period following vaccination. By design, this method artificially reduced the appearance of early adverse events in vaccinated individuals while simultaneously inflating the rate of events in the “unvaccinated” control group. In many COVID-19 vaccine safety studies, individuals were not classified as “fully vaccinated” until 14 days after their second dose of an mRNA vaccine, or at least 14 days post-injection for a single-dose vaccine such as Johnson & Johnson’s Janssen product. This arbitrary waiting period ensured that any adverse events occurring within the critical first two weeks after injection were recorded as happening in “unvaccinated” individuals.
This methodological trick had profound implications for how vaccine safety data was presented to the public. Since most severe vaccine-related adverse events, including anaphylaxis, myocarditis, blood clots, and pregnancy complications, occur within days or weeks of vaccination, reassigning these cases to the "unvaccinated" group created an illusion that serious complications were more common among those who did not receive the vaccine. This method was particularly deceptive in pregnancy safety studies, as early pregnancy loss often occurs within the first trimester, which closely overlaps with the window in which women would still be classified as “unvaccinated” following their first dose. As a result, miscarriages that may have been vaccine-induced were attributed to the unvaccinated population, skewing the data to favor vaccine safety claims.
Another major method of statistical manipulation was the selective use of VAERS data. The Vaccine Adverse Event Reporting System (VAERS) is a passive surveillance system used to track post-marketing vaccine safety signals in the United States. While VAERS is widely recognized as an important tool for identifying potential safety concerns, regulatory agencies and vaccine manufacturers have historically applied inconsistent standards when interpreting its data. When VAERS reports suggested concerning safety signals, such as a sharp increase in pregnancy complications, spontaneous abortions, myocarditis in young men, or blood clotting disorders, these reports were dismissed as unreliable, anecdotal, or coincidental. The CDC and FDA repeatedly downplayed alarming trends, arguing that VAERS data was not designed to establish causation and could be influenced by reporting bias.
However, when VAERS data aligned with pro-vaccine messaging, it was suddenly treated as robust and authoritative evidence of safety. For example, when the CDC and FDA wanted to reassure the public that COVID-19 vaccines did not increase the risk of miscarriage, they cited VAERS data suggesting that pregnancy loss rates post-vaccination were “within normal background rates”—even though the same dataset contained clear spikes in reports of pregnancy loss following vaccine rollout. This double standard allowed public health agencies to cherry-pick findings that supported vaccination while ignoring those that raised legitimate concerns.
The premature termination of clinical trials further contributed to the suppression of safety signals. The Pfizer pregnancy trial (C4591015), which was supposed to be one of the most rigorous investigations into vaccine safety in pregnancy, was cut short before meaningful long-term conclusions could be drawn. Initially planned to enroll 4,000 pregnant women, the study was abruptly downsized to only 348 maternal participants, a sample size far too small to detect rare but serious complications. The trial was eventually discontinued altogether, with Pfizer citing “enrollment challenges” due to the widespread recommendation of COVID-19 vaccination for pregnant women. However, this explanation raises serious ethical questions. If global health authorities had already declared COVID-19 vaccination safe in pregnancy, why was Pfizer unable to recruit enough participants? And why was the trial not expanded to generate more definitive evidence rather than being abandoned altogether?
The consequences of terminating these studies prematurely were far-reaching. Without long-term follow-up, there was no structured effort to evaluate child development outcomes in babies born to vaccinated mothers. No formal studies were conducted to investigate potential immune dysfunction, developmental delays, or long-term neurological effects. Instead of requiring robust long-term data before making sweeping recommendations, public health agencies prematurely declared the vaccine “safe for pregnancy” based on an underpowered and incomplete trial.
The combination of reclassifying adverse events, selectively using VAERS data, and ending clinical trials before long-term data could be gathered ensured that any potential harms associated with maternal vaccination were buried under layers of manipulated statistics and incomplete research. This pattern of obfuscation is not merely a failure of scientific integrity—it is a betrayal of the ethical responsibility to protect pregnant women and their unborn children from poorly studied medical interventions.
This manufactured perception of “safe and effective” vaccines in pregnancy was then amplified by public health messaging that discouraged critical inquiry and vilified medical professionals who sought to raise legitimate concerns. By the time real-world pregnancy data began emerging, showing increases in miscarriage, stillbirths, and menstrual irregularities, the damage had already been done. Women who suffered pregnancy complications post-vaccination were dismissed by their doctors and told their symptoms were “unrelated”. The absence of long-term data on child health outcomes meant that no structured effort was ever made to assess the potential generational consequences of mass maternal vaccination with an experimental mRNA platform.
The techniques used to suppress vaccine safety signals during pregnancy were not errors or oversights—they were intentional choices made by regulatory agencies, pharmaceutical companies, and policymakers who prioritized compliance over caution. These data manipulations shaped public perception, controlled the scientific discourse, and ultimately undermined the ability of women to make truly informed medical decisions.
Without a fundamental shift toward transparency, independent oversight, and genuine scientific accountability, these failures will be repeated in future public health campaigns. The deceptive tactics used to obscure vaccine risks in pregnancy reveal a systemic problem in medical research, one that demands urgent reform before another generation of women and children are subjected to policies based on incomplete and manipulated data.
Violations of 45 CFR 46, the Common Rule, and the Special Protection of Pregnant Women in Research is More Directly Applicable Than Helsinki
The Code of Federal Regulations Title 45, Part 46 (45 CFR 46), also known as the Common Rule, establishes ethical and legal requirements for the protection of human subjects in federally funded research. Within this framework, Subpart B specifically addresses the involvement of pregnant women, fetuses, and neonates in research, outlining stringent safeguards to prevent unethical experimentation and coercion.
In the context of COVID-19 vaccine recommendations for pregnant women, the application of 45 CFR 46 and the Common Rule raises serious concerns about whether proper informed consent was obtained, whether sufficient safety data existed prior to vaccine promotion, and whether public health agencies violated key ethical protections for pregnant research subjects.
Informed Consent Violations Under 45 CFR 46.116
Under 45 CFR 46.116, informed consent is a fundamental requirement for research involving human subjects. This regulation mandates that participants be provided with:
A full disclosure of the risks and benefits of participation.
A clear statement that participation is voluntary.
A right to withdraw from the study at any time without penalty.
A comprehensive explanation of alternative options.
For pregnant women, this requirement is particularly critical, as research must ensure that both maternal and fetal risks are fully disclosed.
In the case of COVID-19 vaccines, these ethical requirements were not met. Public health agencies, hospitals, and employers pressured or mandated vaccination for pregnant women without presenting the true experimental nature of the intervention.
The CDC and FDA explicitly admitted that pregnant women were excluded from the initial clinical trials for COVID-19 vaccines. However, this information was not fully disclosed to pregnant women before they were encouraged—often coerced—into receiving the vaccine.
The long-term effects on fetal development, miscarriage risk, and congenital anomalies were unknown, yet health agencies falsely assured pregnant women that vaccination was “safe at any stage of pregnancy.”
No robust alternative options were presented, despite the fact that natural immunity, antibody testing, and risk-stratified approaches could have provided different pathways for decision-making.
By failing to meet these basic informed consent requirements, public health officials may have violated 45 CFR 46.116, which could constitute an ethical and legal breach of federal research protections.
Special Protections for Pregnant Women Under 45 CFR 46.204
Subpart B of 45 CFR 46 (45 CFR 46.204) specifically states that pregnant women may only be involved in research if the study meets additional safeguards, including:
Preclinical and clinical studies must provide adequate risk assessment data before enrolling pregnant subjects.
The research must present a direct benefit to the pregnant woman and/or fetus.
If risks exist to the fetus, they must be minimal unless the intervention offers a potential direct benefit.
Failure to Meet Safety Prerequisites
COVID-19 vaccines did not undergo proper preclinical and clinical studies on pregnant women before being widely recommended. In direct violation of 45 CFR 46.204, pregnant women were encouraged to take the vaccine despite a lack of preclinical reproductive toxicology data.
Pfizer’s own internal documents (later released under FOIA requests) revealed that the company had insufficient safety data on pregnancy outcomes, yet vaccine campaigns moved forward without caution or proper data transparency.
Animal studies on mRNA vaccines suggested potential risks, including fetal abnormalities, but these concerns were minimized or dismissed by regulatory agencies.
Public messaging failed to acknowledge the true investigational nature of the intervention, violating the principle of full disclosure required under Subpart B of 45 CFR 46.
This disregard for federal research ethics governing pregnant women is unprecedented. Historically, pregnant women have been treated with extreme caution in clinical research, particularly in relation to drug trials. The sudden reversal of this standard for COVID-19 vaccines represents a significant departure from established ethical protections.
Was the COVID-19 Vaccine Rollout an Unregulated Experiment on Pregnant Women?
Under 45 CFR 46.102(l), the definition of research involving human subjects includes any activity where data is collected to develop generalizable knowledge. Given that the COVID-19 vaccines were distributed under Emergency Use Authorization (EUA) and had not completed full safety trials, the widespread push to vaccinate pregnant women effectively constituted a mass human experiment.
Normally, any study involving experimental medical interventions in pregnancy would require Institutional Review Board (IRB) oversight and strict adherence to ethical standards outlined in 45 CFR 46. However, the COVID-19 vaccine campaign bypassed these legal and ethical safeguards by:
Promoting an untested intervention as “safe” without adequate supporting data.
Encouraging pregnant women to take the vaccine without a proper risk-benefit analysis.
Using public mandates and workplace coercion to force compliance, despite the lack of informed consent.
These actions align with what is defined in federal regulations as "research" on human subjects, yet the government did not apply research ethics protocols that would have been required under normal circumstances. This suggests that pregnant women were unwittingly enrolled in a mass clinical trial without regulatory oversight, informed consent, or ethical review—an extraordinary violation of medical ethics.
Consequences of Violating 45 CFR 46: Ethical and Legal Implications
If COVID-19 vaccine recommendations for pregnant women violated 45 CFR 46 and the Common Rule, this raises serious legal and ethical concerns for public health agencies, research institutions, and pharmaceutical companies.
Failure to meet informed consent requirements could expose institutions to legal liability for misleading patients.
Ethical violations under Subpart B could lead to investigations by the Office for Human Research Protections (OHRP), which oversees compliance with 45 CFR 46.
Any research conducted under false pretenses could result in withdrawal of government funding for institutions that violated these federal protections.
Moreover, the use of public health mandates to enforce participation in an experimental intervention—without the full transparency and risk disclosure required under federal law—could constitute a mass breach of human research protections.
Given that pregnant women have historically been shielded from experimental research unless stringent safety criteria are met, the COVID-19 vaccine rollout sets a dangerous precedent where emergency conditions can be used to justify bypassing ethical safeguards.
A Clear Violation of Research Ethics in Pregnancy
The push for COVID-19 vaccination in pregnancy represents one of the most significant violations of 45 CFR 46 and federal human research protections in modern medical history. Pregnant women were actively encouraged—and in many cases coerced—into receiving an experimental medical product without proper safety data, full informed consent, or adherence to regulatory safeguards.
Subpart B of 45 CFR 46 was specifically designed to protect pregnant women and their unborn children from being used as test subjects in poorly studied interventions. However, these regulations were ignored or circumvented in the name of public health policy.
Moving forward, there must be accountability for these ethical violations, including:
A full independent review of COVID-19 vaccine safety policies in pregnancy.
Legal and congressional investigations into whether public health agencies violated federal research protections.
Stronger oversight mechanisms to prevent future abuses of human research ethics.
Unless these violations are acknowledged and addressed, future emergency situations could be used to justify further ethical breaches, undermining public trust in medical institutions and regulatory bodies. The failure to uphold the Common Rule in the COVID-19 vaccine rollout demonstrates that ethical safeguards are only as strong as the willingness of institutions to enforce them.
Silencing Dissent: The Retaliation Against Physicians and Coercion of Pregnant Women
During the COVID-19 pandemic, physicians and scientists who raised concerns about vaccine safety—especially regarding its use in pregnancy—faced severe professional and personal consequences. Rather than fostering an open scientific debate, regulatory agencies, medical boards, and social media platforms actively suppressed dissenting voices, ensuring that only pro-vaccine messaging was allowed to reach the public. Physicians who warned about the lack of adequate safety data, called for more cautious approaches, or reported concerning patient outcomes were censored, vilified, or even stripped of their medical licenses.
Dr. Mary Bowden, an ENT specialist in Texas, was suspended from Houston Methodist Hospital for questioning vaccine mandates and promoting early treatment protocols that diverged from the CDC’s recommendations. Despite treating thousands of patients and publicly advocating for informed consent, she was branded as a spreader of misinformation, with her hospital severing ties over social media statements. Her case was not isolated; it was part of a wider pattern of silencing doctors who challenged the prevailing COVID-19 vaccine narrative.
Dr. Paul Thomas, a pediatrician in Oregon, was another victim of institutional retaliation. He conducted an independent study comparing health outcomes between vaccinated and unvaccinated children in his practice, finding that the unvaccinated group had lower rates of chronic illness. For this, the Oregon Medical Board suspended his license and demanded that he stop practicing medicine. His case sent a chilling message to other physicians: questioning vaccine safety, even with data-driven analysis, could cost them their careers.
Perhaps one of the most egregious examples was Dr. Pierre Kory, a critical care physician specializing in respiratory illnesses, who testified before the U.S. Senate on early COVID-19 treatment options. His work in early intervention strategies and his cautionary stance on vaccine mandates led to widespread censorship on social media. YouTube and Twitter removed his interviews and congressional testimony, branding them as "medical misinformation," despite the fact that his clinical expertise and real-world experience were undeniable.
This institutional suppression was not confined to physicians alone. Pregnant women who refused COVID-19 vaccination also faced direct discrimination, coercion, and denial of services. Many healthcare facilities refused to treat unvaccinated pregnant women, citing policies that restricted care based on vaccination status. There were numerous documented cases of pregnant women being denied medical procedures, fertility treatments, and even routine prenatal care due to their vaccine refusal.
One particularly shocking case involved a pregnant woman in New York who was denied a kidney transplant unless she complied with the hospital's COVID-19 vaccine mandate. Despite the well-established ethical principle that medical decisions—especially for high-risk patients—should be made based on individual risk-benefit analysis, she was left with an ultimatum: take the vaccine or be removed from the transplant list. This represents an alarming departure from patient-centered care, where public health policies replaced individual medical decision-making.
Workplace coercion was another major pressure point for pregnant women. Many private companies, hospitals, and government agencies instituted strict vaccine mandates that left pregnant employees with a devastating choice—comply with the mandate or lose their jobs. This occurred despite the CDC’s own admission that pregnant women were underrepresented in clinical trials and that data on long-term fetal outcomes was lacking.
Some employers went even further by denying paid maternity leave to unvaccinated women or refusing workplace accommodations for pregnant employees concerned about vaccine side effects. This forced thousands of expectant mothers to either comply against their will or face financial hardship. For many, the decision was not truly voluntary—it was made under duress.
Beyond medical discrimination and workplace coercion, social ostracization was weaponized to enforce compliance. Pregnant women who publicly expressed concerns about vaccination were labeled as “anti-vaxxers” and accused of “harming their unborn children” for waiting for more data before making a medical decision. The public pressure to conform, combined with widespread censorship of alternative viewpoints, meant that many women felt isolated, ridiculed, and gaslit for exercising caution.
The persecution of doctors who questioned vaccine safety and the coercion of pregnant women into medical compliance was not just an unfortunate byproduct of the pandemic—it was a deliberate strategy to enforce uniformity and silence dissent. The long-term consequences of this suppression extend far beyond COVID-19; they erode trust in medical institutions, stifle legitimate scientific inquiry, and set a dangerous precedent where compliance is prioritized over informed consent.
Unless these abuses are addressed, future public health policies will continue to rely on coercion rather than transparency, and patients will be denied their fundamental right to make informed medical decisions without fear of retribution.
Conclusion: A Systematic Failure of Science and Ethics
The systemic failures in vaccine safety research for pregnancy were not accidental—they were deliberate.
From the 2009 H1N1 vaccine rollout to the COVID-19 pregnancy trials, public health agencies and pharmaceutical companies suppressed safety concerns, distorted data, and prioritized vaccine uptake over maternal and fetal health.
Without transparency, independent oversight, and accountability, public trust in vaccine safety will continue to erode. The time to demand ethical, rigorous, and truly independent research is now.
Stunning work. Deep bows to you. What a relief to see the exposure of fraud and harm happening on a daily basis now, and in cases like this, with excellent scholarship. (As a mother making medical and vax decisions for three small children in the late 90s and early 2000's, such info was much harder to come by. I had an excellent naturopath who used ethical and reliable research, and I remember the book, Evidence of Harm, being a key source. But professionals as a whole were asleep at the wheel.)
This article was so rich. I placed it within the context of multiple subjects (Covid data integrity, Vaccines generally, and Medicine generally):
Data on Covid injection safety was censored, biased, manipulated, and corrupted.
https://birdseyeviewperspective.substack.com/p/data-on-covid-injection-safety-was
Vaccines Part 1: Corruption, Concealment, Fraud
https://birdseyeviewperspective.substack.com/p/vaccines-part-1-corruption-concealment
Establishment Medicine Part 3: Regulatory & Association Betrayal
https://birdseyeviewperspective.substack.com/p/establishment-medicine-part-3-regulatory
Excellent. This is a chapter in history that will hopefully never be forgotten, but I fear it will. History is easily rewritten in the digital world.