


How The Definition of "Fully Vaccinated" Misleads People on COVID-19 Vaccine Safety & Efficacy: An Explanation For CNN's Drew Griffin
Received one dose only? You're Unvaccinated. Two doses? Wait another 14 days. If you survive, congratulations. You're fully vaccinated.

Everywhere I turn I see claims of COVID-19 vaccine efficacy and safety from studies in the US that defy all logic and reason. The results are the opposite of those seen in the UK and Israel. Here, I go through claims made that have led to the belief that the COVID-19 vaccine is safe, and effective, and explore factors that have been carefully manipulated to produce that misperception.
Moderna Vaccine’s 95% Efficacy
“An Epidemic of the Unvaccinated”
“Boosters are Effective”
“Pfizer’s Vaccine >90% Effective (ahem, “Useful”) in Children Aged 5-12”
“Zero deaths and serious adverse events from COVID-19 vaccines”
I recently watched a CNN segment in which Drew Griffin's beliefs are absolutely contradicted by the facts that CDC defines "Fully Vaccinated" as people who have made it to the second week (14 days) after their second dose. The fact that anyone who experiences adverse events or dies, and anyone who is diagnosed with COVID-19 before 2 weeks have passed after their second dose are not counted as deaths in the "fully vaccinated". That means that a person who is vaccinating might not be considered “Fully Vaccinated” until five weeks after their first dose.
It is shameful for Griffin to not know this fact, and the impact of this fact on calculations of breakthrough infections vs. re-infections vs. infections in the "unvaccinated". Therefore, I outline in detail for Dr. Griffin the key information he needs to know.
Moderna Vaccine’s 95% Efficacy. In January 2021, I published an article in Robert F. Kennedy’s online magazine, The Defender. The article, entitled “Discrepancies in Moderna’s FDA Report Demand Answers”, I offered the following analysis:
“In contrast to what Moderna reported to the U.S. Food and Drug Administration (FDA) in the early months of COVID-19, its mRNA vaccine is not an established technology. It is new. As a new, experimental vaccine, it deserves close and objective scrutiny.
Moderna reports 94.5% efficacy. The “efficacy” of vaccines is understood to be a measure of the effectiveness of the vaccine on an ideal population, and differs from “effectiveness,” which is how well a vaccine manages to induce evidence of immunity in the real population upon which it is being used.
Moderna reported to the FDA (Zhang, 2020) efficacy as the ratio of the rate of SARS-CoV-2 infection in the vaccinated (16 infected out of 28,068 vaccinated) to the rate of infection in the placebo group (275 infected out of 27,956 given placebo).
Close inspection of Moderna’s data made public ahead of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBAC) meeting that was scheduled for Dec. 17, 2020, however, reveals that among the vaccinated, an additional 81 participants and 118 among the placebo participants developed a COVID-19 diagnosis between the first and second shots. These participants were determined to be ineligible for the second dose and removed from the study.
By my calculations, these additional cases shift the vaccine efficacy from 94.5% to 75.4%.
If a chemotherapy agent is being tested against another cancer treatment, the deaths that occur between scheduled treatment rounds must be counted. It is misleading not to count these additional cases of COVID-19 in the Moderna vaccine trial — the 94.5% efficacy is not based in clinical reality even for an ideal population.”
“Efficacy” here, and in Moderna’s use, means the ability of the vaccine to prevent a certain condition in an ideal population. They excluded people with health conditions - for example, metabolic syndrome, diabetes, autoimmune disorders.
What does this mean for the rest of us? Well, given that they reported 95% efficacy, when it should have been 74.4%, means that the vaccine coverage needed for herd immunity was going to be way low.
Fauci’s initial 66-67% coverage needed for herd immunity was tied to Moderna’s 95% efficacy. Fauci never should have come in that low, for two reasons. First, Moderna’s 95% efficacy - the performance of the vaccine in an ideal population - was not, as I showed, 95%. Second, that efficacy could not have been expected to translate into effectiveness - the performance of the vaccine in a non-ideal population, the one with people with metabolic disorder, diabetes, and autoimmune conditions.
Even though later trials used the same tactic of excluding people who got COVID-19 before the second dose, the official estimate of vaccine effectiveness in fact took a nose-dive in the 60-70% range in studies on sample groups representative of the full adult population, and yet to this day public health servants still cite the vaccine as “effective as 95% as in the Moderna trial”.
The data from Barnstable, Massachusetts tell a different story. This was an MMWR report that showed that 74% of new cases in Barnstable County were in those who had been exposed to COVID-19 vaccines. The report actually used the term “exposed”, and they also showed that the RT-PCR cycle threshold distribution of the two groups, “exposed” and “unexposed” were not different. This was the report that led CDC Director Rochelle Walensky to warn that people who were vaccinated still needed to wear a mask and to socially distance.
Almost all of the new cases were Delta variants. Using the 74% of cases in the vaccinated number, it is possible to estimate vaccine efficacy against the Delta variant. Assuming an R0 of 2.6, the VE of all vaccines combined in use in Barnstable County for single-dose exposed persons was almost precisely zero. When estimated for persons exposed to two doses, the VE falls to -0.26, or =26%. People in Barnstable County who are “fully vaccinated” have a 26% increased risk of COVID-19 diagnosis.
It is worth pointing out that because the clinical trials used PCR to determine the case status in the patients considered “vaccinated” and those considered “unvaccinated”, the actual efficacy estimates were likely invalid given they should have been calculated after a certain number of COVID-19 cases had occurred. With false positive rates of PCR ranging from 11% to over 90%, the actual disposition of patients in the vaccinated and unvaccinated arms of the trial is anyone’s guess.
“An Epidemic of the Unvaccinated”
CDC’s Director, Rochelle Walensky, said yesterday that CDC’s definition of “fully vaccinated” might need to be updated due to boosters. This semantic gameplay would back the population into mandated boosters if the OSHA rule comes through. Remember that it was Walensky who overruled the FDA’s decision to not recommend boosters for all. So now, we are facing the confusing situation in which people w/vaccine cards are no longer “fully vaccinated”. As we have seen, the efficacy of the current vaccines against extinct variants might be reasonably high (whatever it is), but the efficacy against extant variants seems to be in question. So, with eternal boosters, perhaps no one will ever be considered “Fully Vaccinated” in the US under CDC’s ever-changing definition.
CDC: When You’ve Been Fully Vaccinated https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html
The accuracy of the claim that the new cases in the US are occurring primarily in the unvaccinated hinges entirely on the CDC’s definition of “Fully Vaccinated”. We know that people who have had two doses are not considered “Fully Vaccinated” until day 14 after their second dose. So, when new cases occur in the partially vaccinated, they do not count toward cases in the vaccinated. There is significant evidence that COVID-19 vaccination may impair the immune system for a short period of time following administration; in particular, the likelihood of a SARS-CoV-2 infection, or an infection by any other respiratory virus or bacterium may be more likely following vaccination. In animal trials on SARS and MERS viruses, close relatives of SARS-CoV-2, and in studies in humans of the RSV virus, this phenomenon was called “disease enhancement”. If disease enhancement is occurring after the first dose, or within two weeks following receipt of the second dose, the CDC’s semantics will bias the case count data and make it appear as if those exposed to vaccines have a lower risk of COVID-19 infection than those who are unvaccinated.
Proof of this type of statistical manipulation in action can be found in a report from the OKLAHOMA COVID-19 WEEKLY REPORT Weekly Epidemiology and Surveillance Report September 19-25, 2021, which, after reporting more new cases in the unvaccinated than in the vaccinated, dropped this fact into a footnote of at table:
“**Vaccine breakthrough cases is (sic) defined as an individual with a COVID-19 positive laboratory results (PCR/Antigen) and documentation of COVID-19 vaccination that meets the definition of fully vaccinated. (Individuals are considered fully vaccinated ≥2 weeks after receiving the last dose in the COVID-19 vaccine series.)”
Due to this sleight-of-statistical-hand, we will need to revisit all of the clinical studies and non-peer reviewed press releases on the safety and efficacy of COVID-19 vaccines as well as the CDC’s non-peer-reviewed MMWR reports and re-estimate vaccine efficacy, breakthrough cases, and vaccine safety.
“Boosters are Effective”
The claims that boosters are effective begs the question: effective at what? Preventing transmission of SARS-CoV-2? No. Reducing deaths due to COVID-19? No. Reducing hospitalization of patients with positive PCR results (true positives + false positives combined)? Yes. However, remember that people are not considered “boosted” until fourteen days after the second dose. Unless COVID-19 cases in those waiting for fourteen days to be counted are included in the calculation of breakthrough cases, we cannot know the true efficacy of boosters.
Pfizer’s Vaccine >90% Effective (ahem, “Useful”) in Children Aged 5-12
News reports tell us that “kid-size doses of Pfizer’s Covid-19 vaccine appear safe and nearly 91% effective at preventing symptomatic infections in 5- to 11-year-olds”.
The Phase 2/3 trial had one=month safety follow-up, and yet the same new source touts “The shots could begin early next month — with the first children in line fully protected by Christmas — if regulators give the go-ahead.”
The Pfizer website describes the trial as “the first of a pivotal trial”. The doses were spaced 21 days apart - meaning that children were not considered “vaccinated” until five weeks after their initial exposure.
It is noteworthy that the incidence of COVID-19 in children is so low that the trial had to accrue patients from four countries. It is also noteworthy that the trial did not undergo peer review; in fact, the company published the results in a press release, which included caveats that the release includes “forward-looking statements”, meaning they put a positive spin on the contents of the press release to encourage investors.
Among those forward-looking statements?
“In participants 5 to 11 years of age, the vaccine was safe, well tolerated and showed robust neutralizing antibody responses.”
The press release does not specify if the vaccination produced neutralizing antibodies against the initial Wuhan SARS-CoV-2 virus, which is extinct, or the more recent variants, such as the Delta variant.
Their less-than forward-looking statements included:
“There is a remote chance that the vaccine could cause a severe allergic reaction
A severe allergic reaction would usually occur within a few minutes to one hour after getting a dose of the vaccine. For this reason, vaccination providers may ask individuals to stay at the place where they received the vaccine for monitoring after vaccination
Signs of a severe allergic reaction can include difficulty breathing, swelling of the face and throat, a fast heartbeat, a bad rash all over the body, dizziness, and weakness
If an individual experiences a severe allergic reaction, they should call 9-1-1 or go to the nearest hospital
Myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the lining outside the heart) have occurred in some people who have received the vaccine. In most of these people, symptoms began within a few days following receipt of the second dose of the vaccine. The chance of having this occur is very low. Individuals should seek medical attention right away if they have any of the following symptoms after receiving the vaccine:
chest pain
shortness of breath
feelings of having a fast-beating, fluttering, or pounding heart
Side effects that have been reported with the vaccine include:
severe allergic reactions; non-severe allergic reactions such as rash, itching, hives, or swelling of the face; myocarditis (inflammation of the heart muscle); pericarditis (inflammation of the lining outside the heart); injection site pain; tiredness; headache; muscle pain; chills; joint pain; fever; injection site swelling; injection site redness; nausea; feeling unwell; swollen lymph nodes (lymphadenopathy); diarrhea; vomiting; arm pain
These may not be all the possible side effects of the vaccine. Serious and unexpected side effects may occur. The vaccine is still being studied in clinical trials. Call the vaccination provider or healthcare provider about bothersome side effects or side effects that do not go away.”
The FDA has determined that the “study” was not large enough to have detected myocarditis - and yet Pfizer has not updated their report to their investors on this fact.
Pfizer would have use vaccinate 28 million children on one months’ safety data and a study that was not large enough to detect even a well-recognized serious adverse event.
“Zero deaths and serious adverse events from COVID-19 vaccines.
The world knows about myocarditis following COVID-19 vaccination, and we have known about it for some time. In June 2021, Tom Shimabukuro gave a presentation to ACIP, the Advisory Committee on Immunization Practices. This was a key meeting at which ACIP would vote to recommend or not recommend that COVID-19 vaccine for teens.
Shimabukuro reviewed data from the Vaccine Safety Datalink - the VSD - a taxpayer-subsidized resource to which only a handful of people are allowed to have unrestricted access. In those data, he reported zero (0) serious adverse events and zero (0) deaths from the COVID-19 vaccines in the United States.
Shimabukuro’s presentation followed a review of myocarditis and pericarditis by a CDC employee, who, in the Q&A, reported that the signal of increased risk of myocarditis in males relative to females in older children (teens) and also in younger children.
In his presentation, Shimabukuro made a point on one slide to highlight myocarditis:
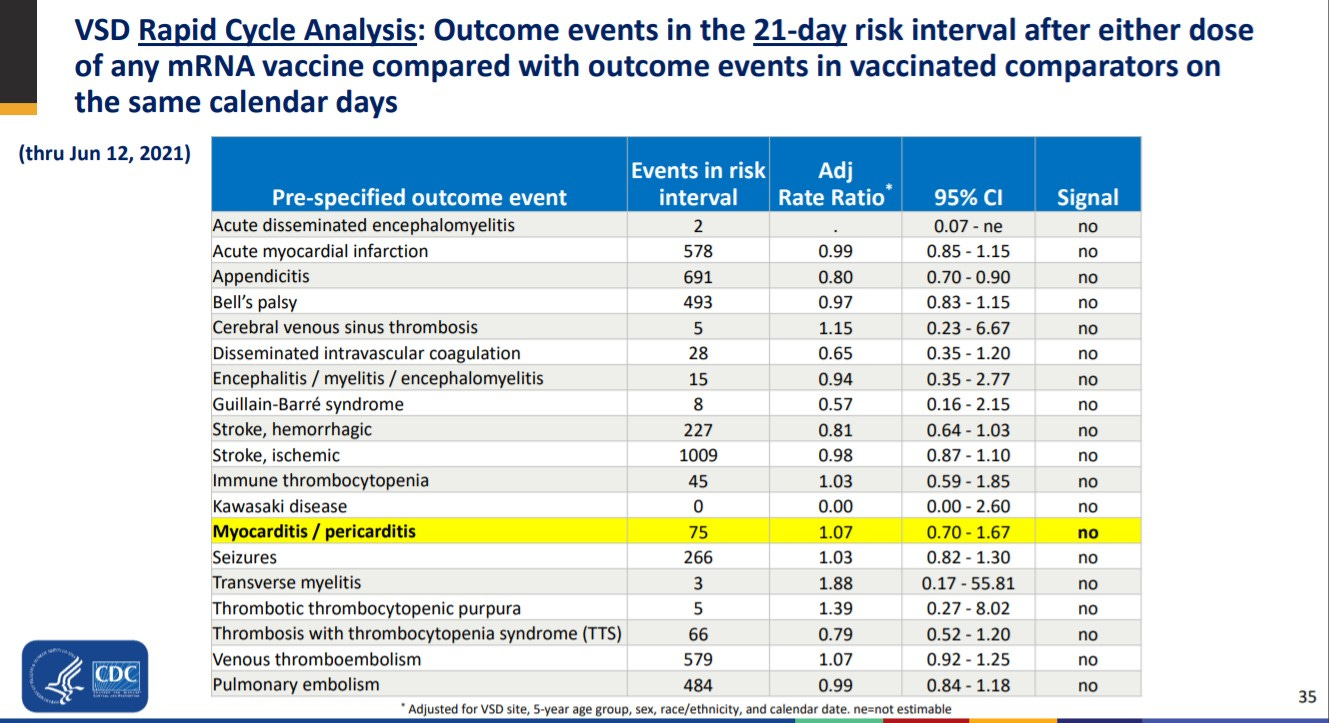
It will be important to know whether Shimabukuro used the CDC’s twisted definition of “Fully Vaccinated”. If he did, then all of the events following the receipt of the first dose and those following the second dose on days 0-13 did not count as occurring in the vaccinated, which would be absolutely misleading.
Two days later, FDA issued a warning on myocarditis and pericarditis risk in male teens following COVID-19 vaccination in spite of Shimabukuro’s presentation. The signal for myocarditis has been established reproducibly by independent analysts. This demonstrates at the very least that VSD - and Dr. Shimabukuro - do not provide “Pharmacovigilance”.
Throughout his presentation, Shimabukuro uses the euphemism “immunization”, showing a lack of knowledge on the fact that “exposure to vaccine” does not equal “immune”, especially in this setting with a rapidly evolving mRNA virus.
In his discussion of VAERS data, Shimabukuro reminds the attendees that “a report to VAERS does not necessarily mean that the vaccine has caused a health problem”, but he failed to also report that “This caveat does not mean that the vaccine has not caused a health problem”.
Data from Ontario, Canada show an increase in myocarditis over time - increases from baseline - as vaccination increased over time - a population-level dose-dependent response not expected unless causality was in play.
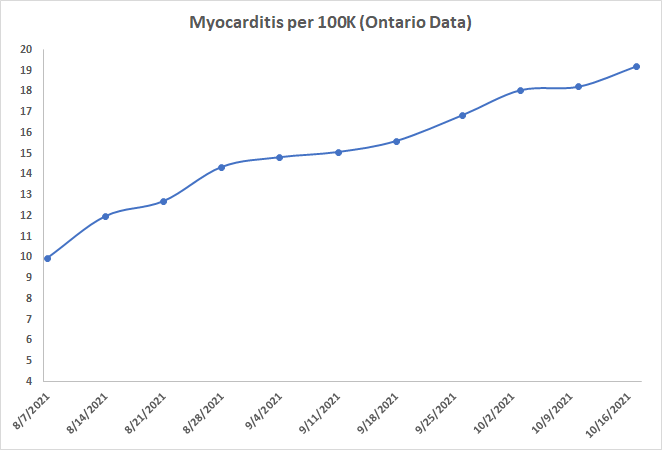
These data show a range of rates of myocarditis trending toward 20 per hundred thousand. Shimabukuro’s reported his rate estimates at 7 per million. I stand by my conclusion that we do not have anything close to vaccine safety monitoring in the United States.
See: mRNA COVID-19 Vaccination and Development of CMR-confirmed Myopericarditis, https://archive.md/pvggn
Shimabukuro’s analysis of myocarditis using VAERS used data up to June 11, 2021. The VAERS analysis separated results following dose 1 and dose 2; the results consistently showed increased risk with the second dose, again, indicative of causality and perhaps pathogenic priming.
Evidently, those reporting to VAERS did not get the memo that those suffering myocarditis following exposure to vaccination should not be considered vaccinated until five weeks after their initial dose.
Conclusions
In the NVICP, causality determination often requires adverse events or deaths following a vaccine to be observed within 8 weeks of the receipt of the vaccine (often using rates beyond 8 weeks as a baseline, which can be higher than the national baseline rates, making that practice also bogus). To delay designation of a vaccinated person as “vaccinated” until up to five weeks after the initial dose is a brazen statistical manipulation to bury perception of adverse events and deaths from COVID-19 vaccination. It is a shameful practice and must not only be stopped: its effects must be reversed.
The public deserves to see efficacy re-calculated, as well as all rates of break-through cases, rates of reinfection cases, and new case rates all reported assuming that the individuals who have been exposed to COVID-19 vaccines, even a single dose, are “vaccinated”. Otherwise, the effect of the vaccine itself is never actually studied, and the relative risk of COVID-19 diagnosis in the vaccine-exposed and the vaccine-unexposed will never be known.
Now that boosters are here, no one may ever be counted as "fully vaccinated". This sick, twisted perversion of logic and reason does not jive with reality, and people are going to get hurt needlessly. With draconian policies putting people’s jobs on the line, their very livelihood, this is far, far more than risk of vaccine injury or death. The definition of groups being studied must be changed to “vaccine exposed” and “vaccine naive”.
If the negative efficacy estimate from the data from the Barnstable report holds, then new breakthrough cases combined with the expected surge in “cases” due to false positives in the millions who may opt to be tested instead of vaccinating will lead to a fifth surge in COVID-19 that dwarfs the peak of the pandemic. The US will have more new “cases” of COVID-19 than the rest of the world combined… that will be a sure sign that something is truly rotten in the United States of America.