


COVID-19 "Rates" Must Adjust for Testing Rates and the DEADLY False Positive Rate. UNLESS SEQUENCED TO CONFIRM OR ALSO TESTED FOR BACTERIAL PNEUMONIA, PEOPLE WILL DIE FROM PCR FALSE POSITIVE RESULTS.
FDA and CDC's Mandy Cohen Must Issue a Warning Against Use of PCR Only as a Diagnosis of COVID-19. We know all of the moving parts of the sham. It's not an error if they try to repeat it.

HEADSUP: THE PROBLEM IS PEOPLE WITH OTHER RESPIRATORY ILLNESSES WILL BE TREATED AS COVID-19 AND WILL DIE FROM BACTERIAL PNEUMONIA. MOST PEOPLE WHO DIED ON VENTILATORS DIED FROM BACTERIAL PNEUMONIA. THEY WON’T RECEIVE ANTIBIOTICS AND OTHER TREATMENTS AND WILL DIE FROM SEVERE BACTERIAL PNEUMONIA AND SEPSIS. READ ON.
You’ve likely seen the ramp-up of pushing for masking at the same time as reports of increases in “cases”, with images like this from the CDC:
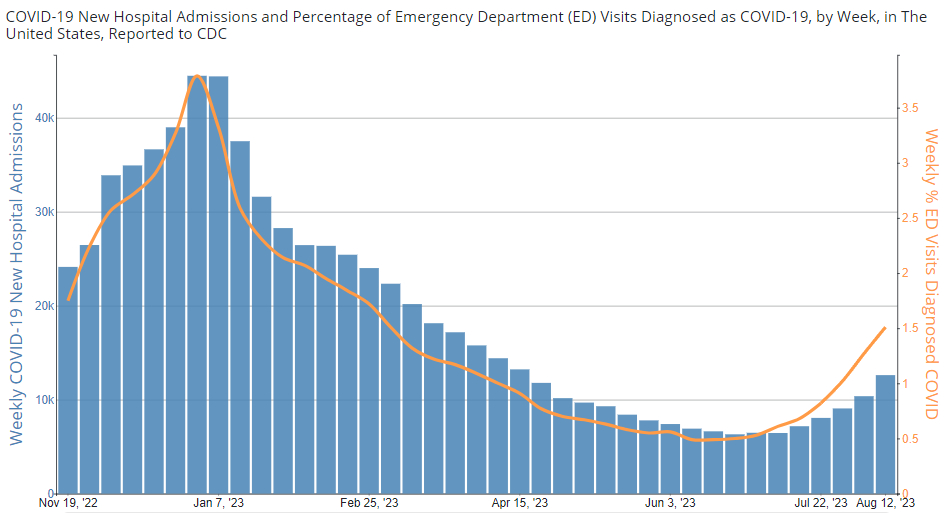
This is accompanied by messaging like “COVID-19 hospitalizations up 22% - hospitalizations not cases” and of course just looking at the data the orange curve is levitating above the data bars, and the alleged “22%” is actually about 0.1% absolute increase. CDC continues to stretch the truth under Mandy Cohen’s direction.
Also, the raw counts tell us that 12,000 people in the US are hospitalized WITH COVID-19 test positive results, not FROM COVID-19.
That’s a whopping 12,000/335,283,774 x 100 = 0.003579% of all people in the US.
There are 920,000 hospital beds in the US, so we’re looking at 1.3% of people in available hospital beds testing positive for COVID-19. Driven by false positives. Not impressive.
Testing Rates Drive These Numbers But CDC Stopped Collecting Testing Rates
There’s a huge issue that remains to be addressed and that’s the problem of testing rates and false positive rates. Data like these must be adjusted for testing rates. They could be worse, or better, we have no clue because CDC just publishes the raw counts.
They stopped collecting PCR testing rates on 9/21/2022:

The data also must be adjusted for the PCR false positive rates - that is, the percentage of cases that test positive that are, in fact, false.
Here is a statement you can expect if testing rates shoot up: “I tested positive again and I just had COVID last month”.
No. Just no.
Sadly, true rates are knowable at any time just by doing Sanger sequencing on the amplicons from PCR amplifications. Any hospital can do this. IPAK NAATEC Consortium member Dr. Sin Hang Lee has generously provided the protocols and primers for that:
Lee SH, McGrath J, Connolly SP, Lambert J. Partial N Gene Sequencing for SARS-CoV-2 Verification and Pathway Tracing. Int Med Case Rep J. 2021 Jan 11;14:1-10. doi: 10.2147/IMCRJ.S291166. PMID: 33469388; PMCID: PMC7810684.
He and I have been warned about this problem since March 2020.
THE PROBLEM IS PEOPLE WITH OTHER RESPIRATORY ILLNESSES WILL BE TREATED AS COVID-19 AND WILL DIE FROM BACTERIAL PNEUMONIA. MOST PEOPLE WHO DIED ON VENTILATORS DIED FROM BACTERIAL PNEUMONIA. THEY WON’T RECEIVE ANTIBIOTICS AND OTHER TREATMENTS AND WILL DIE FROM SEVERE BACTERIAL PNEUMONIA AND SEPSIS.
Here are some key references:
Lee, S-H. 2022. Evidence-Based Evaluation of PCR Diagnostics for SARS-CoV-2 and the Omicron Variants by Sanger Sequencing. Science, Public Health Policy & the Law ←IPAK JOURNAL WEBSITE
ABSTRACT. Both SARS-CoV-2 and SARS-CoV initially appeared in China and spread to other parts of the world. SARS-CoV-2 has generated a COVID-19 pandemic causing more than 6 million human deaths worldwide while the SARS outbreak quickly ended in six months with a global total of 774 reported deaths. One of the factors contributing to this stunning difference in the outcome between these two outbreaks is the inaccuracy of the RT-qPCR tests for SARS-CoV-2, which generated a large number of false-negative and false-positive test results that have misled patient management and public health policy-makers. This article presented Sanger sequencing evidence to show that the RT-PCR diagnostic protocol established in 2003 for SARS-CoV can in fact detect SARS-CoV-2 accurately due to the well-known nonspecific PCR amplification of DNAs with similar sequences. Using nested RT-PCR followed by Sanger sequencing to retest 50 patient samples collected in January 2022 and sold as RT-qPCR positive reference confirmed 21 (42%) were false-positive. Although the other 29 positive isolates were categorized as Omicron variant by partial sequencing of the N gene, and the RBD and the NTD of the S gene, 9 (31%) showed focal to complete sequencing failure in the S gene segments due to multi-allelic SNPs. During the course of the study, an Omicron variant isolate containing a BA.1 NTD and a BA.2 RBD in its S gene was also detected. Routine partial S gene sequencing of all PCR-positive samples can timely discover multi-allelic SNPs and viral recombination in the circulating variants for investigation of their impacts on vaccine efficacies, therapeutics and diagnostics.
False-positive COVID-19 results: hidden problems and costs - The Lancet Respiratory Medicine
Even a correct diagnosis can lead to death, with ineffective and harmful hospital protocols.
So we have two failures of the medical system leading to deaths attributed to this virus.
1. You really do have covid, and they withhold effective treatments and administer dangerous treatments that kill you.
2. You don't have covid, but they withhold treatment for what you do have that could save your life, and instead administer dangerous treatments that kill you outright, or you just die for lack of treatment for what you actually have.
I started sending evidence of the PCR, Bacterial pneumonia, Ventilator protocols, test + nursing home release by state governors with the conclusion of coordinated "mass murder" to my local investigative newspaper reporter. They previously covered my small part as a agitator against a case of high profile municipal corruption in the late 90's which led to state receivership for the City and me getting targetted for several decades, lol. Since this whole debacle is tied into energy, finance and social engineering, I expect a hard landing once the fantasy meets the physical reality. Prepare accordingly. If you experience interference adopt a recovery approach.. create resilience, form a Junto, learn nonviolent resistance and other forms of self defense.