

Counting Integrity: What Do We Do When A Bioethicist Cannot Count?
Art Caplan was once caught on video declaring war on his fellow Americans those who want to refuse vaccines. Now he wants them to trust his math.

So-called “bioethicist” Art Caplan’s MedPage Today editorial claims that most American children receive “about 30 doses” of vaccines across 16 diseases. By contrast, Secretary Robert F. Kennedy Jr.’s HHS team, through the January 2026 Høeg/Kulldorff report, documented a far more complex and expansive exposure count: up to 92 discrete vaccine events, and many more when considering strain-level detail. This article reconstructs the counting systems behind those conflicting claims, dissects CDC 2025 vaccine schedule assumptions, and demonstrates—using real biological, scheduling, and economic logic—why Caplan’s framing fails both analytically and ethically.
Caplan’s Fractured Arithmetic of Vaccine Counting
Caplan’s assertion of “about 30 doses” contains no definition of what a “dose” is. A shot? A disease-target? A product component? The CDC’s own immunization guidance makes no such simplification. The reality is that there are at least four separate, equally valid vaccine exposure metrics:
Product-based doses: Every time a vaccine is administered, regardless of combo structure.
Component targets: Every unique disease targeted, regardless of how many in one shot.
Strain-level (valency): Each serotype, strain, or viral type targeted (e.g., PCV20 = 20).
Taxon/species-based: Each biologically distinct pathogen.
Caplan does not disclose his metric, but by excluding annual flu, COVID, HPV, MenACWY, and collapsing all multivalents into a single count, we reconstruct that he is counting only around 30 injections, stopping at adolescence.
By contrast, Høeg/Kulldorff’s “up to 92” refers to component doses, including:
Routine childhood series
Annual flu and COVID boosters
Full HPV and MenACWY series
RSV-mAb
Maximum possible schedules (e.g., 3-dose HPV, 3-dose rotavirus)
This metric aligns with CDC coverage policies, CPT billing codes, and biological targeting logic.
CDC 2025 Schedule: Real Numbers, Real Complexity
An exact tally of vaccine exposures from birth to age 18 under the 2025 CDC schedule reveals the discrepancy. For example:
HepB: 3 product doses = 1 species = 1 component = 1 strain
DTaP: 5 product doses × 3 targets = 15 components
PCV20: 4 doses × 1 component = 4, but targets 20 serotypes
HPV9: 2 or 3 doses = 9 strains × 2 = 18 strain-level exposures
COVID-19: 1/year × 18 years = 18 components (or strains)
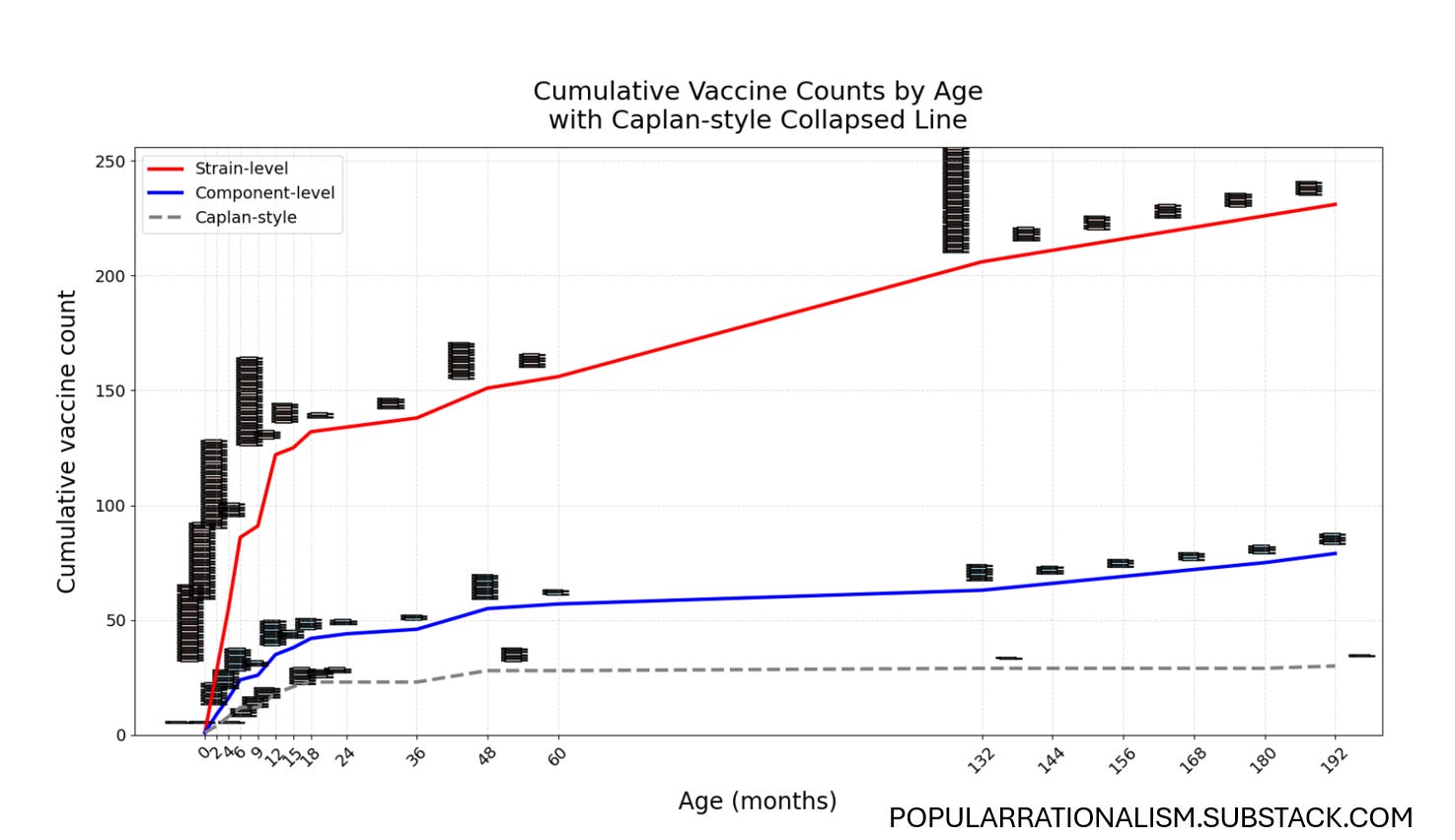
Figure 1: Stacked Syringes Do Not Lie. Three Counting Methods
This figure shows cumulative vaccine exposures over time, across three counting methods, with each new injection represented by flat syringe icons stacked above the curve. Caplan’s counting method minimizes reported exposures. Why?
Caplan’s Ethical Framing Fails Its Own Logic… And Could Cost Pediatricians Large Sums of Profit
Caplan argues that Kennedy’s policy violates the ethical principle of beneficence by allowing disease risk to increase. But ethical analysis requires transparency about both benefits and risks. Caplan omits:
Risk of intussusception from rotavirus
Febrile seizures from MMRV
Myocarditis from mRNA COVID vaccines
Aluminum exposure associations with asthma (VSD 2023)
Mention of product warnings that all vaccines come with a risk of death.
He makes no comparison at all to the risks of serious disease, hospitalization of deaths from other countries that seem to get by with far fewer jabs.
He also fails to note that no CDC schedule-wide safety trial has ever been conducted, and multiple vaccines were approved without saline placebo trials. Informed consent, in Caplan’s view, is apparently only valid if it reinforces his side.
Comparative Schedules: U.S. vs Peer Nations
The HHS report shows that the U.S. recommended more diseases and more product doses than any other nation. Denmark vaccinates against 10–11 diseases. The U.S. vaccinated against 18, not counting COVID. When Caplan says the U.S. is “in line” with peers, he ignores this comparative data and the vaccine landscape of nations like France, Japan, Germany, and the U.K.
MMRV, Combination Products, and Dose Compression Games
Caplan’s count ignores how strain-compressed products like MMRV and Pentacel alter perception. Giving MMR + Varicella separately = 2 shots. MMRV = 1 shot. But both contain 4 live virus strains. Similarly, Pentacel collapses DTaP + Hib + IPV into 1 injection.
Combo products reduce needle counts, not biological exposures. Counting them as “1 dose” ignores reality.
Financial Incentives and Pediatric Reimbursement
Caplan omits that pediatricians are compensated per administration. Under CPT codes 90460/90461, each component adds revenue. Vaccine manufacturers, providers, and CMS all count components, not injections, when billing.
Providers and CMS bill per dose administered, using product codes. Components are used to adjust administration reimbursement when counseling is documented.
Administration CPT codes:
90460: For the first antigen in a vaccine administered during a counseling session
90461: For each additional antigen/component in the same vaccine, billed as add-ons
Caplan’s math would upend the entire Medicaid and VFC billing system if applied seriously.
He omits his own conflict of interest statement, as well.
The True Exposure Ledger
Thanks to comprehensive data modeling from the CDC schedule and biological products, we now know:
Strain-level exposure: 231 by age 18
Component-level: 79
Species-level (‘disease’): 16
Caplan-style injection collapse: ~30
Each method is internally consistent. But only Caplan presents his total without disclosing his assumptions.
Conclusion: Disclose or Disqualify
If Caplan wants to participate in the policy conversation, he must disclose what he counts and why. Until then, his critique of HHS’s up-to 92-dose claim is nothing more than rhetorical sleight of hand. Science must clarify. Bioethics must quantify. Policy must account.
The future of vaccine trust is harmed by the minimization of risk perception. That train left the station long ago.
Caplan still has yet to receive the memo.
Make sure he does. Please share this on X, Facebook, TruthSocial, Bluesky, LinkedIn or anywhere parents hang out so they are not mislead by this unethical bioethicist.
Visit me on X. We are doing more spaces these day. Love to hear from you.

Thankful for you, Dr JLW, for your brain’s ability and your extensive experience to navigate through this succinctly and clearly for the benefit of all.
To say that Caplan is a troll or can’t count is going way too easy on him. In most professions, if someone presented such an inept, obviously misleading, analysis, he would no longer be considered be considered an expert or even trustworthy. Once you lie / mislead like he has in this instance (think of the damage he may be doing), you should be treated as an deceitful charlatan - probably bought out by big Pharma.